

Continuous Intraoperative Neurophysiological Monitoring (IONM) for Early Detection and Prevention of Pedicle Screw related Spinal Cord Injury
May 08, 2019
Faisal R. Jahangiri, MD, CNIM, D.ABNM, FASNM
Paper presented at:
- American Society of Neurophysiological Monitoring (ASNM) Annual Meeting, Chicago, IL. May 2014.
- The Neurodiagnostic Society (ASET) & Southern Society of Electroneurodiagnostic Technologists (SSET) Co-sponsored Annual Meeting, Asheville, NC, Aug 2014.
- International Society of Neurophysiological Monitoring (ISIN) Annual meeting. Istanbul, Turkey. Oct 2014.
Objective:
This case report illustrates the benefit of utilizing intra-operative neurophysiological monitoring (IONM) with continuous somatosensory (SSEP) and motor evoked potentials (TCeMEP) during pedicle screw placement in scoliosis correction surgery.
Introduction:
Pedicle screw placement has a high risk of damaging the motor and sensory pathways due to its close proximity to the spinal cord. An early detection and prevention of injury can be achieved by utilizing Somatosensory Evoked Potentials (SSEP) and Trans Cranial electrical Motor Evoked Potentials (TCeMEP) during a scoliosis surgery.
Case Report:
A 19-year-old female with scoliosis was presented for surgery. After intubation, electrodes were placed for ulnar in upper and posterior tibial nerve SSEPs in lower extremities. Electrodes for EMG and TCeMEP were placed in thenar-hypothenar, quadriceps, gastrocnemius, tibialis anterior, abductor hallucis and extensor hallucis brevis muscles. Total intravenous anesthesia was used with propofol 200 mcg/kg/min and remifentanil at 0.5mcg/kg/min. Inomed ISIS IOM Neuromonitoring machine (Inomed Medizintechnik GmbH, Emmendingen, Germany) was used IONM for this surgery. Baseline SSEP and TCeMEP responses were present in all limbs.
Four pedicle screws were placed on left side of T6, T9, T12 and L1 followed by placement of four screws on the right side of the same spinal levels. After placing the last screw at right L1, surgeon was immediately informed of loss of TCeMEP signals bilaterally in lower extremities. Surgery was paused. TCeMEP responses returned to baseline in left lower limb but remained absent in right lower limb. All screws were removed on right side with no improvement. A wake-up test was performed which was negative in her right leg. Later, left side screws were also removed. Blood pressure was increased from MAP of 80 to 96 mmHg. An 8.0 mg of I.V. hydrocortisone was given intraoperatively. There was no improvement in right lower limb TCeMEP responses. Then, 400 mg of hydrocortisone was given post-operatively.
Surgeon was advised to stop the surgery and proceed for MRI and follow-up. SSEP signals remained stable in all four extremities. The surgical correction was cancelled.
Post-operative:
Patient was taken to the MRI suite intubated. MRI revealed intramedullary spinal cord ischemic changes at T11. This was a result of an insult to a small vessel near right T11 level from the pedicle screw. After extubation, patient was unable to move her right lower extremity with flaccid paralysis. She also complained about severe burning in her left lower extremity. Patient was taken for rehabilitation exercises. One week post-op, patient was moving hip flexors and two week later had a full motor function bilaterally.
Conclusions:
Real-time IONM was useful in early identification of spinal cord injury. Significant changes were seen in TCeMEP within 2 minutes, without any change in SSEP. We highly recommend utilizing continuous TCeMEP and SSEP monitoring during pedicle screw placement for prevention of injury to the spinal cord. Any delay in running motor evoked potentials during pedicle screw placement may result is loss of TCeMEP signals at an unknown instance. In this case, patient would have been paralyzed post-operatively without the use of IONM.
References:
- Skinner SA, Rippe DMJ Clin Neurophysiol. 2012 Dec;29(6):493-501.
- Parker et al. J Neurosurg Spine. 2011 Aug;15(2):130-5
- Isley MR, Zhang XF, BalzerJR, Leppanen RE. Neurodiagn J. 2012 Jun;52(2):100-75.
- Jahangiri FR, Sheryar M, Al Behairy Y. 2014. Early detection of pedicle screw-related spinal cord injury by continuous intraoperative neurophysiological monitoring (IONM). Neurodiagn J. 54:323– doi: 10.1080/21646821.2014.11106817.
- Jahangiri FR: Surgical Neurophysiology: A Reference Guide to Intraoperative Neurophysiological Monitoring (IONM). Second Edition. Jahangiri FR (ed): CreateSpace. Independent Publishing Platform, Charleston, SC, USA; 2012.
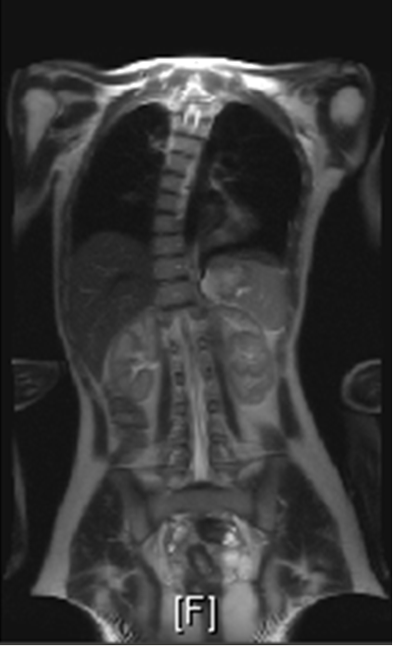
Figure 1: Pre-operative MRI showing Scoliosis.
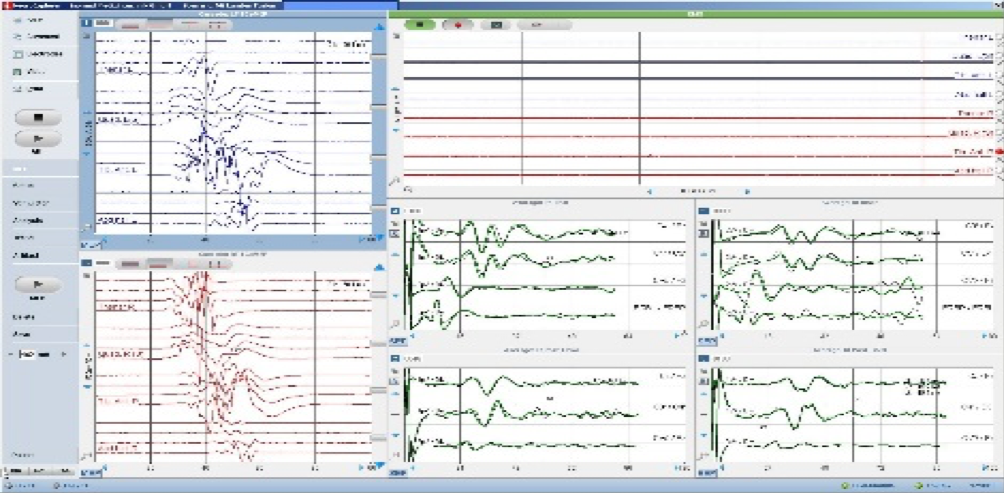
Figure 2. Baseline TCeMEP, SSEP & EMG Data
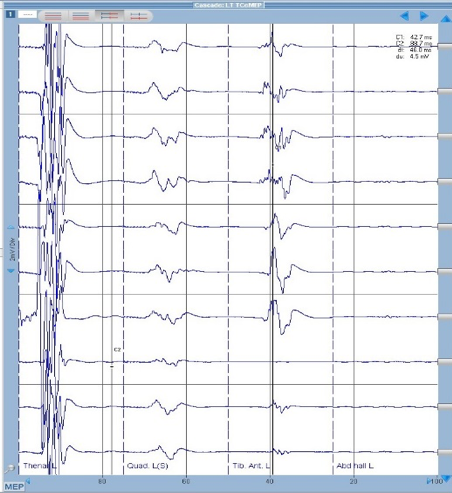
Figure 3. Left Lower TCeMEP loss & recovery
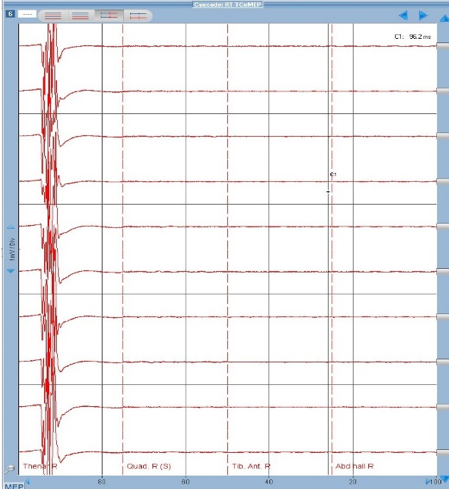
Figure 4. Right Lower TCeMEP loss, No recovery
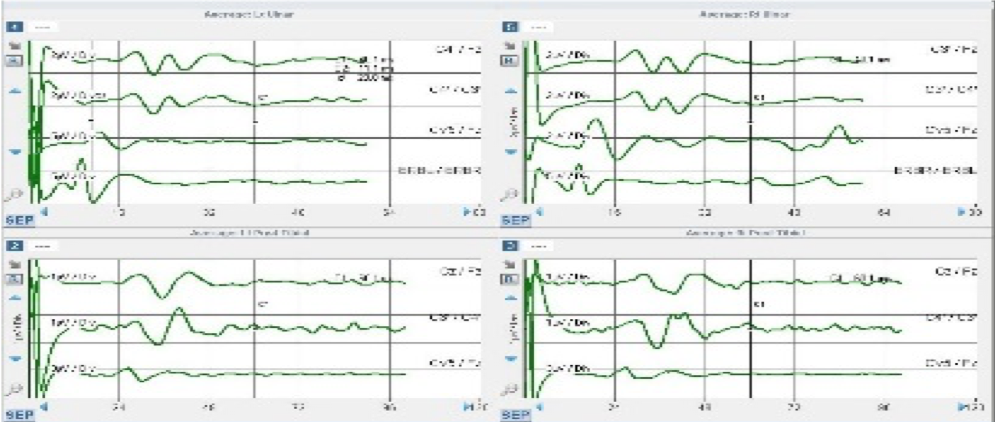
Figure 5. Ulnar & Posterior Tibial Nerves SSEP Closing Data
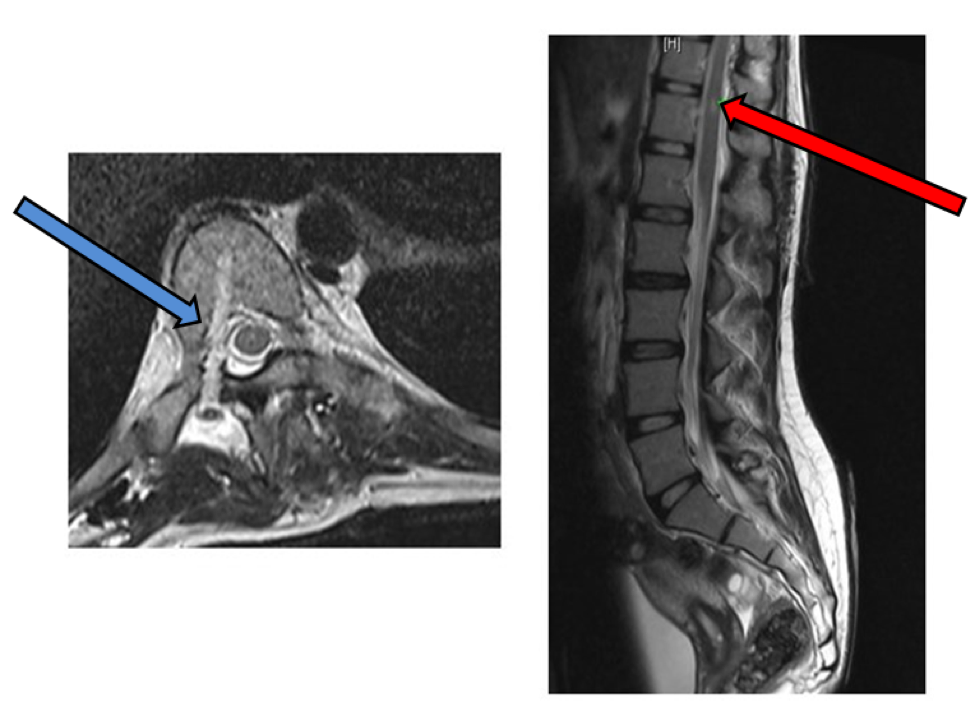
Fig. 6. Post-operative MRI: (Left) cross-sectional view: a pedicle screw course with a cerebrospinal fluid (CSF) filled cavity showing a medial pedicle wall breach (blue arrow). (Right) Lateral view showing ischemic insult at T11/T12 junction (red arrow).