

Improving the Patient Outcomes by Utilization of Intraoperative Neurophysiological Monitoring (IONM) During Spine Surgery: Case Report
July 29, 2019
Faisal R Jahangiri, MD, CNIM, D.ABNM, FASNM
Introduction: Sensory and motor functions are at risk during spine surgeries. This case report demonstrates the utilization of Intraoperative Neurophysiological Monitoring (IONM) during a spine surgery for an early detection of a possible nerve or spinal cord injury.
Methods: A retrospective analysis of neurophysiological monitoring data from a spine instrumentation procedure was performed. A 73-year-old female, with history of lower right sided back and hip pain was admitted with spinal stenosis and lumbar region neurogenic claudication. Co-morbidities included hypertension, arthritis, and bilateral foot neuropathy. Neuromonitoring paradigm included upper and lower extremity somatosensory evoked potentials (SSEPs) as well as spontaneous and triggered electromyography (EMG) from the lower extremity muscles bilaterally. Train of four (TOF) was also recorded from the abductor hallucis muscle as well for monitoring the level of muscle relaxant.
Results: During the case, the screws were placed in the spine pedicle and were tested with triggered EMG (t-EMG). One of the lumbar screws at left L4 had a lower than accepted threshold. The surgeon was immediately informed, and the screw was removed and readjusted. The EMG test value improved after the recommended adjustment. Postoperatively no neurological deficit was noted due to tiemly identification and repositioning of the malpositioned pedicle screw.
Conclusion: In this surgical procedure, we were able to acquire t-EMG. T-EMGs can be attempted in surgeries that put the function of the spinal cord and peripheral nerves at risk. If low screw threshold was not identified by intraoperative neuromonitoring, it may have resulted in a breached pedicle causing damage to the spinal cord or the adjacent nerves. Hence, patient would have post-operative muscle weakness, numbness, severe pain, or foot drop, etc.
More study is needed to establish better statistical methods, better modality efficacy, and a better understanding of intraoperative countermeasures that may be employed when an alert is encountered to prevent impending neurological sequelae.
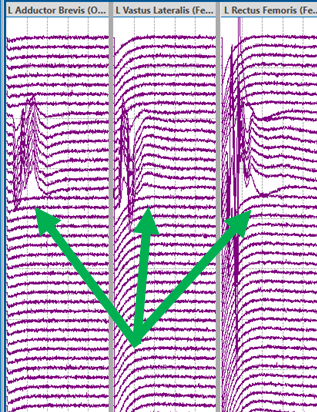
Figure: A low threshold triggered EMG (t-EMG) response from the left L4 pedicle (Green arrows).
__________________________________________________________
References:
1. Jahangiri FR, Sheryar M, Al Behairy Y. Early detection of pedicle screw-related spinal cord injury by continuous intraoperative neurophysiological monitoring (IONM). Neurodiagn J. 2014 Dec;54(4):323-37.
2. Eager M, Shimer A, Jahangiri FR, Shen F, Arlet V. Intraoperative neurophysiological monitoring (IONM): lessons learned from 32 case events in 2069 spine cases. Am J Electroneurodiagnostic Technol. 2011 Dec;51(4):247-63.
3. Parker SL, Amin AG, Farber SH, McGirt MJ, Sciubba DM, Wolinsky JP, Bydon A,Gokaslan ZL, Witham TF. Ability of electromyographic monitoring to determine the presence of malpositioned pedicle screws in the lumbosacral spine: analysis of 2450 consecutively placed screws. J Neurosurg Spine. 2011 Aug;15(2):130-5.
4. Jahangiri FR, Sherman JH, Holmberg A, Louis R, Elias J, Vega-Bermudez F. Protecting the genitofemoral nerve during direct/extreme lateral interbody fusion (DLIF/XLIF) procedures. Am J Electroneurodiagnostic Technol. 2010 Dec;50(4):321-35.