

Language Mapping During Awake Brain Surgeries
June 04, 2018
Faisal Riaz Jahangiri, MD, CNIM, D.ABNM, FASNM1,2,
Arshad A. Siddiqui, MBBS, FCPS, MSc, FINR2
1Axis Neuromonitoring LLC. Richardson, TX, USA; 2Dept. of Neurosurgery, Neuroscience Institute, Hamad Medical Corporation, Doha, Qatar.
Awake brain surgery is a preferred technique for a lesion near or involving the language areas in brain. It allows us to test function before, during and after the resection. It also minimizes the overall risk of the surgery.
Intra-operative neurophysiological monitoring (IONM) is performed during awake surgeries involving Broca’s and Wernicke’s areas for assessing language function. The purpose of the IONM is to minimize any post-operative language deficits by identifying the language cortex and immediately alerting the surgeon with proximity with cortical stimulation, which allows the surgeon to modify the surgical approach. In brain surgeries, the IONM is used to guide the surgeon by mapping sensory, motor and language areas of the nervous system.
IONM with sensory & motor mapping, as well as Electrocorticography (ECoG) is a well-recognized method to identify the central sulcus and surrounding eloquent tissues to decrease the risk of neurological injury. IONM provides a real-time feedback to the surgeon during resection and is advantageous over pre-operative imaging modalities. The goals for performing neuromonitoring are (1) preservation of vital brain functions (such as language and motor), (2) precise localization of sensory, motor, language & epilepsy area is highly variable and (3) maximizing extent of resection while avoiding any new deficits.
The most important factor for predicting minimum post-operative language deficits is the distance of more than 10.0 mm resection margin from the language site. Cortical tumor resection can be maximized with minimal permanent language deficits by utilizing a multimodality cortical language mapping.
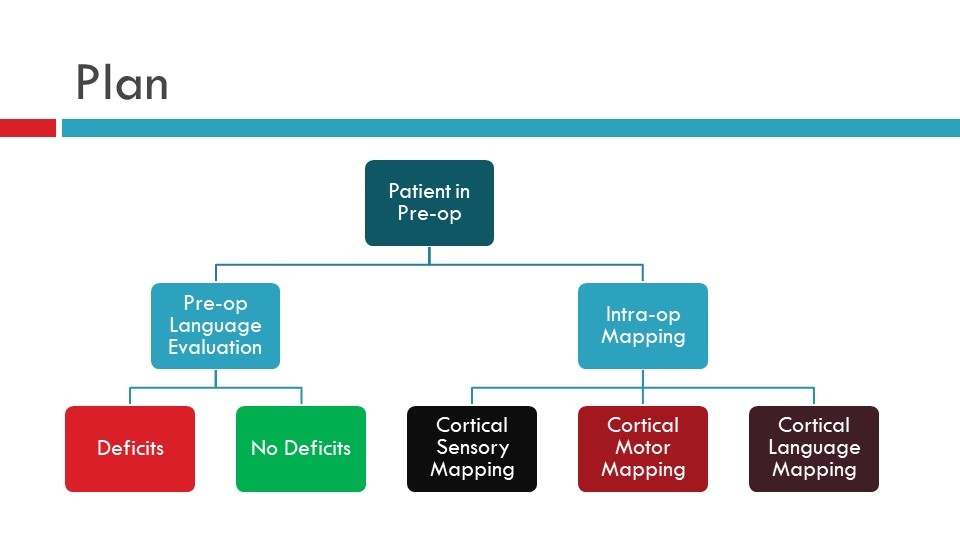
Figure 1. Preoperative Monitoring Plan for Language Mapping
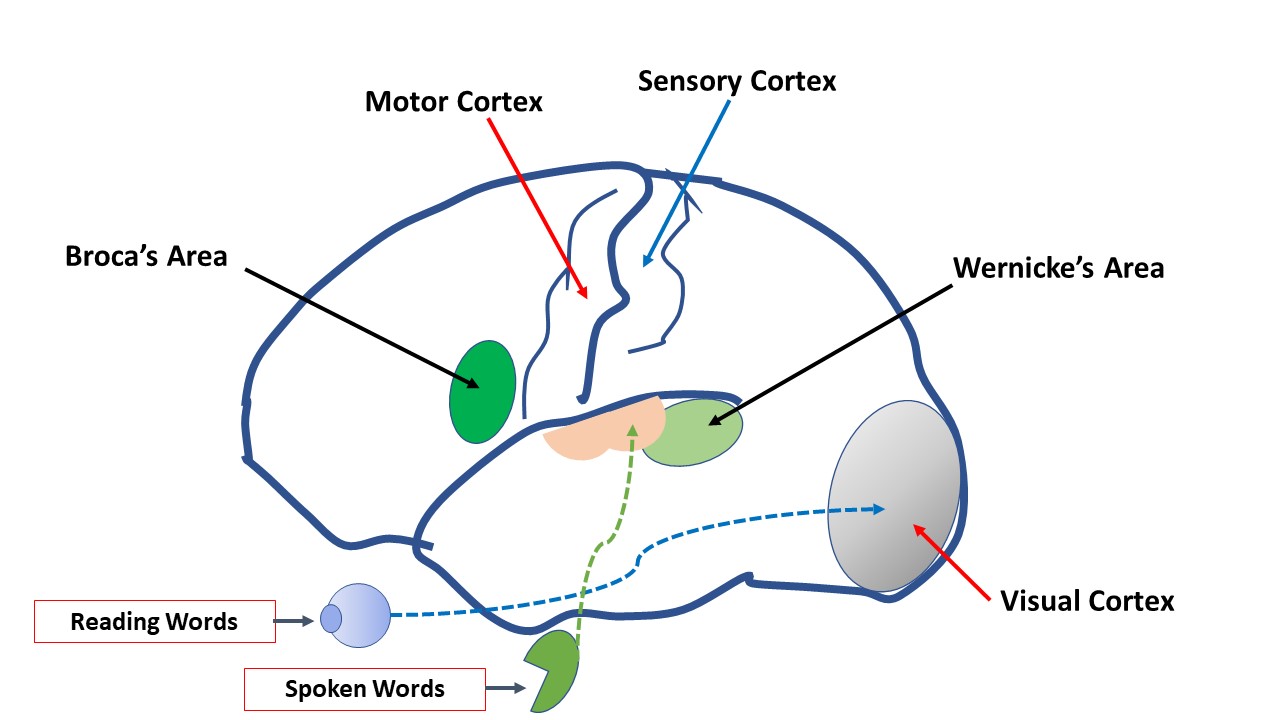
Figure 2. Sensory, Motor and Language areas of the brain.
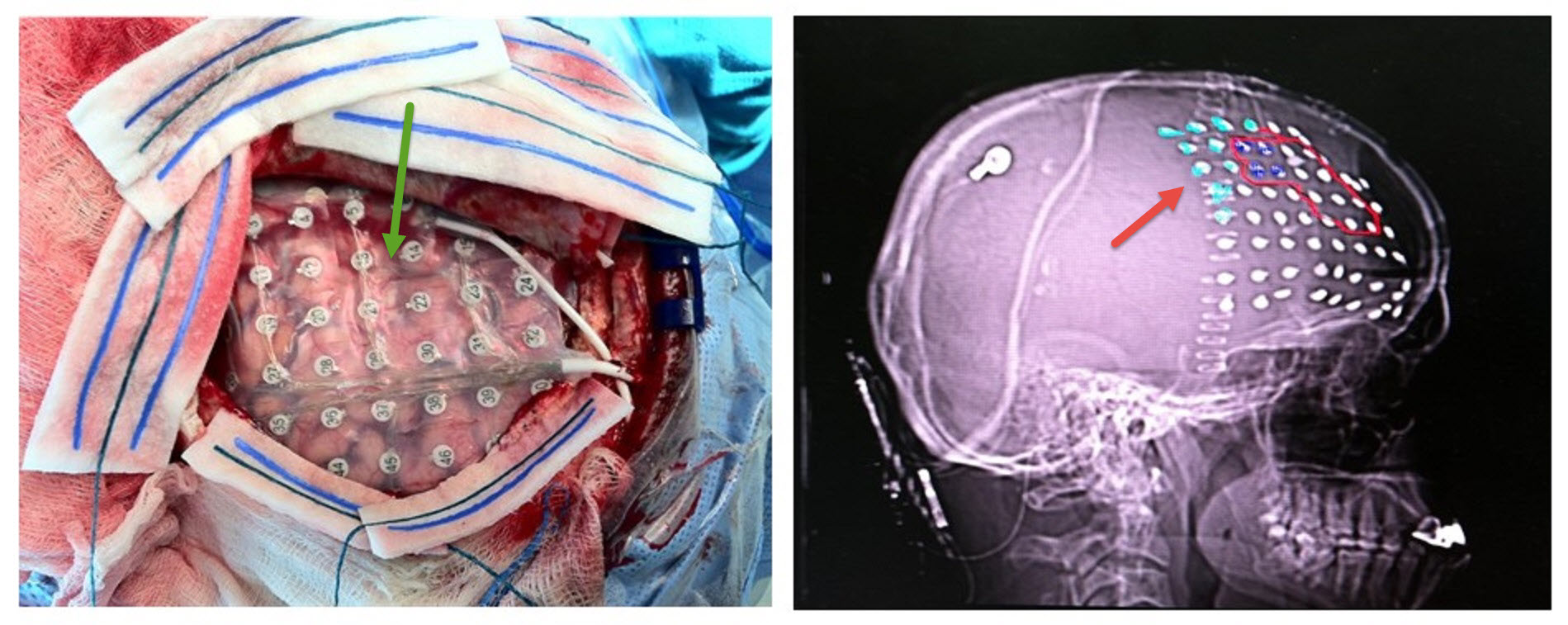 Figure 3.(Left) A with 64 contact (8x8) grid placed on exposed cortex to localize the sensory, motor and language area of the cerebral cortex. (Right) A C-Arm view of the brain with 64 contacts (8x8) grid placed on the exposed cortex. Light blue are Post-Central, and Red outline are Pre-Central contacts.
Figure 3.(Left) A with 64 contact (8x8) grid placed on exposed cortex to localize the sensory, motor and language area of the cerebral cortex. (Right) A C-Arm view of the brain with 64 contacts (8x8) grid placed on the exposed cortex. Light blue are Post-Central, and Red outline are Pre-Central contacts.
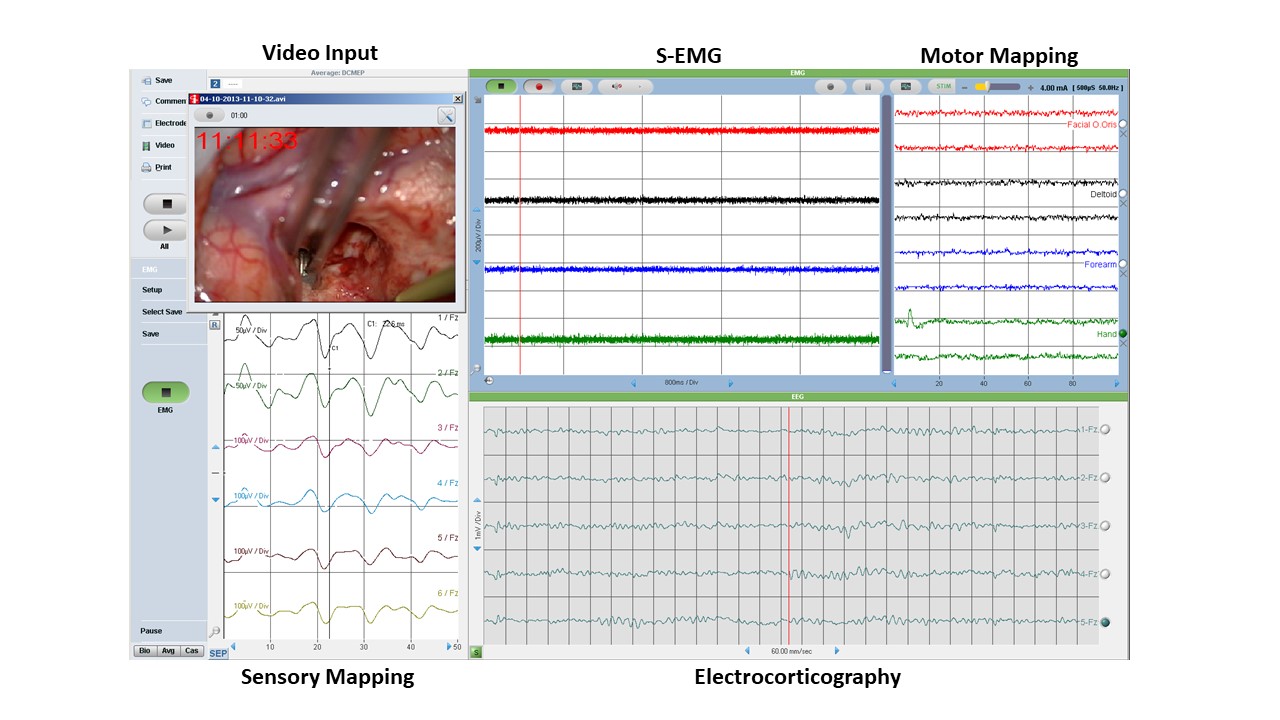
Figure 4. Multimodality Intraoperative Neurophysiological Monitoring (IONM) data showing spontaneous Electromyography (s-EMG), Sensory Mapping (Phase Reversal), Motor Mapping (DECS: Direct Electrical Cortical Stimulation, Electrocorticography (ECoG) and Video input from the operating microscope.
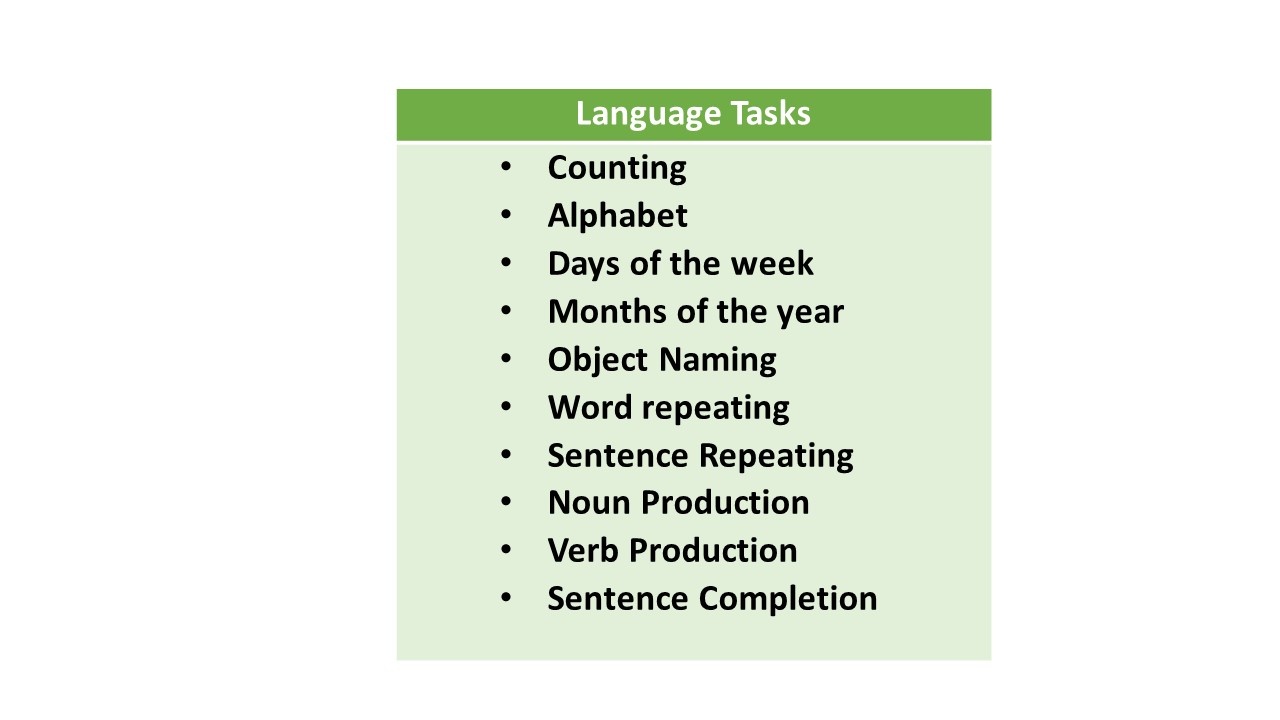
Table 1. Language tasks used to for language evaluation preoperatively and intraoperatively.