

Multimodality Intraoperative Neurophysiological Monitoring (IONM) for Preventing Cranial Nerve Injuries during High Risk Brain Surgeries Faisal R. Jahangiri, MD, CNIM, D.ABNM, FASNM1,
August 07, 2018
Introduction:
There are 12 pairs of cranial nerves (CN). All of them can be monitored except CN I (Olfactory). Various monitoring techniques (also known as Modalities) that can be utilized intraoperatively include spontaneous Electromyography (s-EMG), triggered Electromyography (t-EMG), Cranial Nerves Motor Evoked Potentials (CN-MEP), Nerve Action Potentials (NAP), Visual Evoked Potentials (VEP), Somatosensory Evoked Potentials (SSEP) (CN V and CN VII) (Fig. 1) and Brainstem Auditory Evoked Potentials (ECoch, AN-CAP, BAEP). CN II (Optic) is a sensory nerve which can be monitored intraoperatively by visual stimulation by flash goggles and recording from the retina (ERG) and visual cortex (VEP) (Fig. 2). CN V (Trigeminal) has a sensory division which is monitored for Trigeminal SEP (TSEP). CN VIII (VestibuloCochlear) is also a sensory nerve which can be monitored by auditory stimulation. Factors effecting BAER response may include N2O, hypothermia and inhalational agents. Multilevel auditory responses are recorded from the tympanic membrane/cochlea (Electrocochleography: ECoch) (Fig. 3), directly from the auditoring nere (Auditory Nerve Compound Action Potentials: AN-CAP) and the braintem (BAEP) (Fig. 4) when preservation of hearing is a high priority.
The remaining CNs are motor and can be monitored intraoperatively by spontaneous (s-EMG) (Fig.5 and Fig.6) and triggered EMG (t-EMG) (Fig.7) . Reasons for monitoring CN during high risk brain surgeries include protecting CN from any damage during the surgical procedure. It also provides real-time feedback to the surgeons, helps in identification and mapping of the CN course, evaluation of the CN function and localization of the damaged nerves. EMG responses can be visualized and are audible as well. Various perioperative factors affecting CN EMG, MEP and VEP responses may include muscle relaxants, inhalational agents, hypothermia, ischemia, etc. CN-MEP can be used to evaluate the integrity of the corticobulbar tracts (Fig. 8). TIVA with no muscle relaxant is the ideal anesthetic regimen for monitoring surgeries involving cranial nerves. Various types of intraoperative insults include mechanical, ischemic, electrical and chemical insults. Monopolar or bipolar stimulations can be used for nerve identification and mapping. Monopolar stimulation is more sensitive and less specific. Whereas, bipolar stimulation is more specific and less sensitive.
Conclusion:
Multimodality intraoperative neurophysiological monitoring can be effectively utilized in preventing injuries to cranial nerves during brain surgery procedures. Optic (CN II) and Vestibulocochlear (CN VIII) nerves can be monitored by visual and auditory brainstem responses for the preservation of the vision and hearing. Cranial nerves III (Oculomotor), IV (Trochlear), V (Trigeminal), VI (Abducens), VII (Facial), IX (Glossopharyngeal), X (Vagus), XI (Spinal Accessory) and XII (Hypoglossal) can be monitoring intraoperatively by s-EMG and t-EMG. The surgeon can decide to limit the tumor resection by the changes in neurophysiological responses. This minimizes any post-operative neurological deficits due to surgical manipulation of the tumor involving the upper and lower cranial nerves. Intraoperative monitoring of CN II-XII can be done effectively and with high confidence without causing any risk to the patient safety.
Intraoperative Neurophysiological Monitoring (IONM) helps in better patient outcomes by minimizing risks related to the functional status of the nervous system during surgical procedures. An IONM alert to the surgical team during the surgery can help them to identify the cause and take an immediate corrective action.
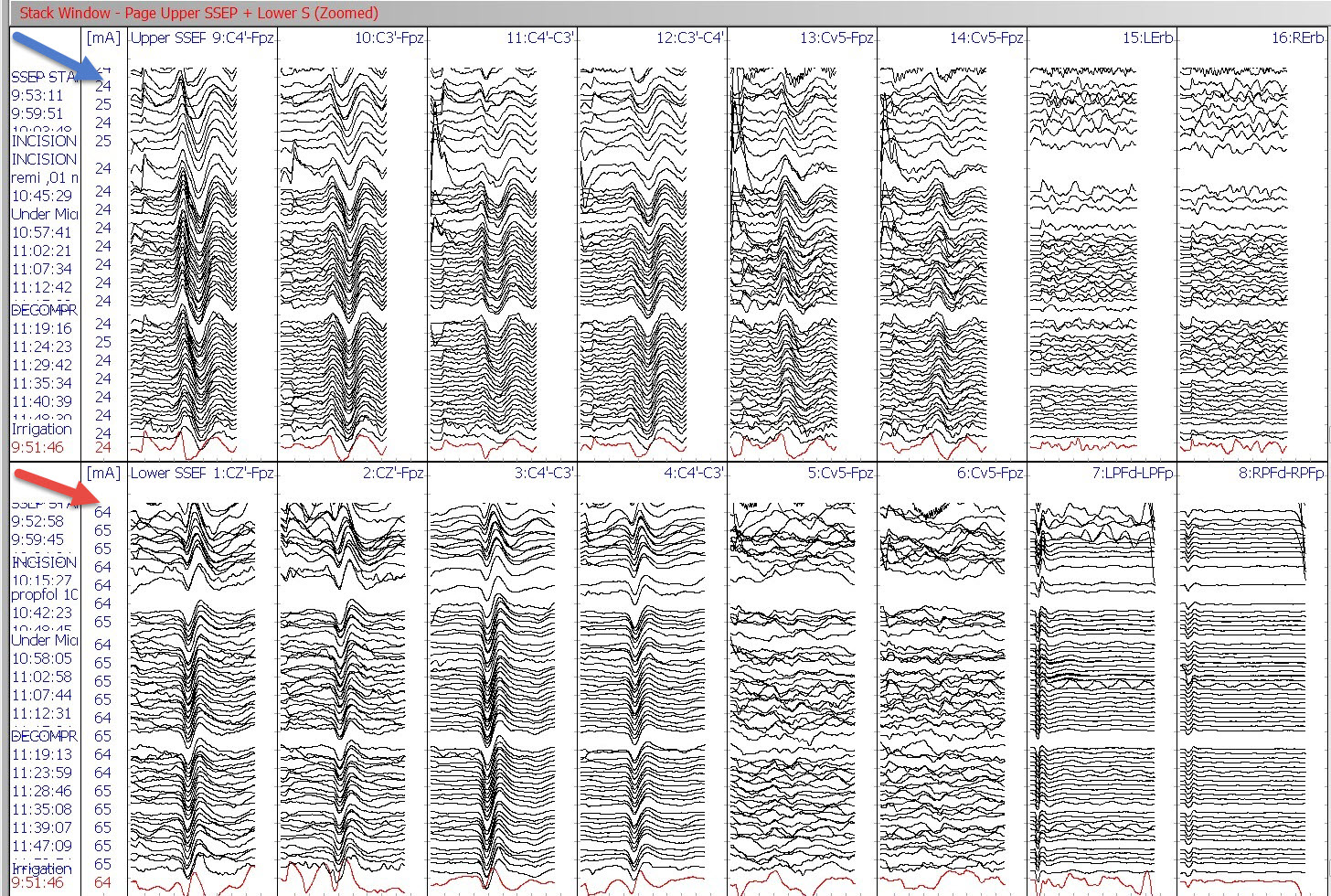
Figure 1: Somatosensory Evoked Potentials (SSEP) stack data bilaterally recorded from scalp, subcortical and peripheral sites by Median nerve stimulation at the wrist (blue arrow) and Posterior Tibial nerve stimulation at medial ankles (red arrow).
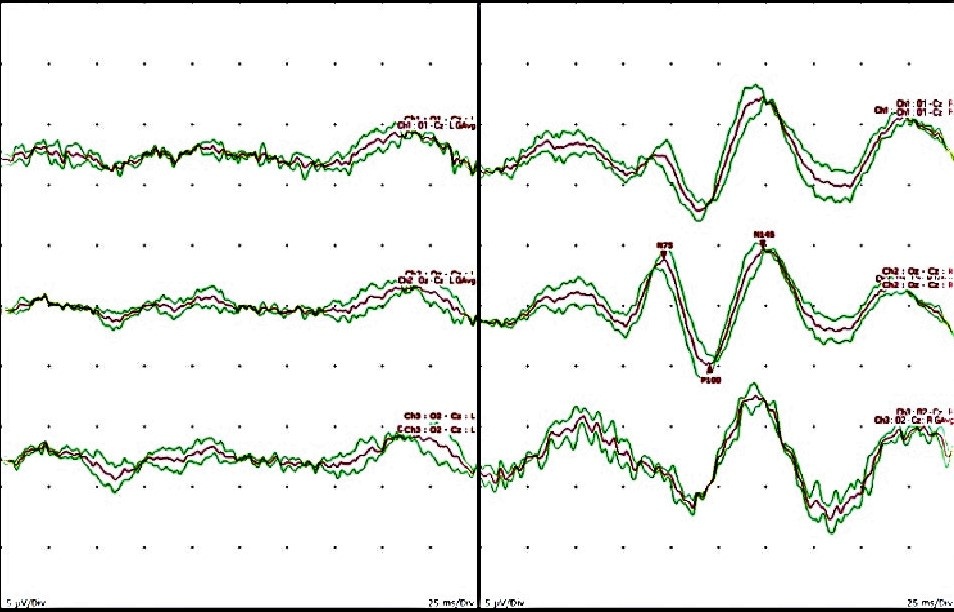
Figure 2: Visual Evoked Potentials (VEP) [Cranial Nerve II]. Left: Absent Flash VEP (FVEP) responses due to loss of vision pre-operatively in the left eye. Right: Reliable FVEP responses present in response to right eye stimulation.
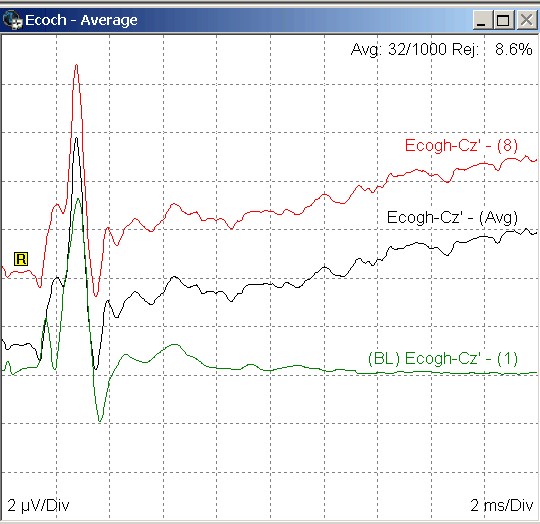
Figure 3: Electrocochleogram (ECoch) with Cochlear Microphonics (CM), Summation Potentials (SM) and Compound Action Potentials (CAP) [Cranial Nerve VIII] recorded from right tympanic membrane.
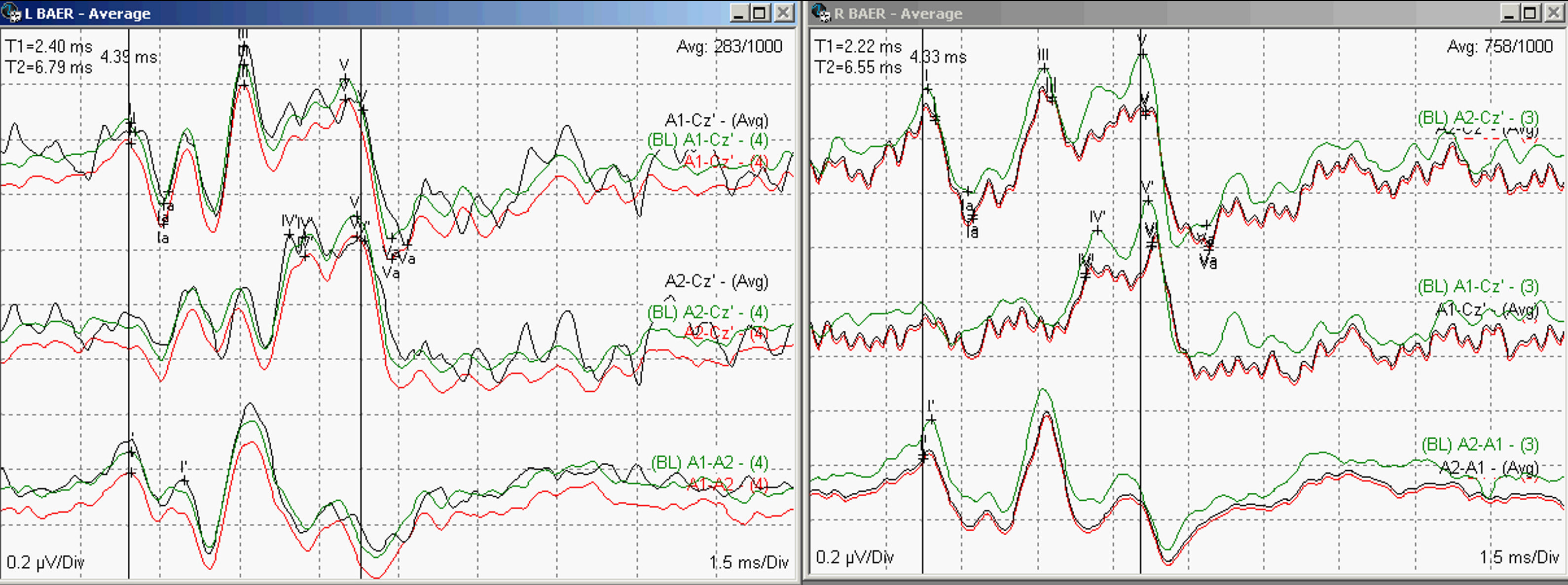
Figure 4: Brainstem Auditory Evoked Potentials (BAEP) [Cranial Nerve VIII] recordings in response to left and ear stimulation (Waves I, III and V present bilaterally).
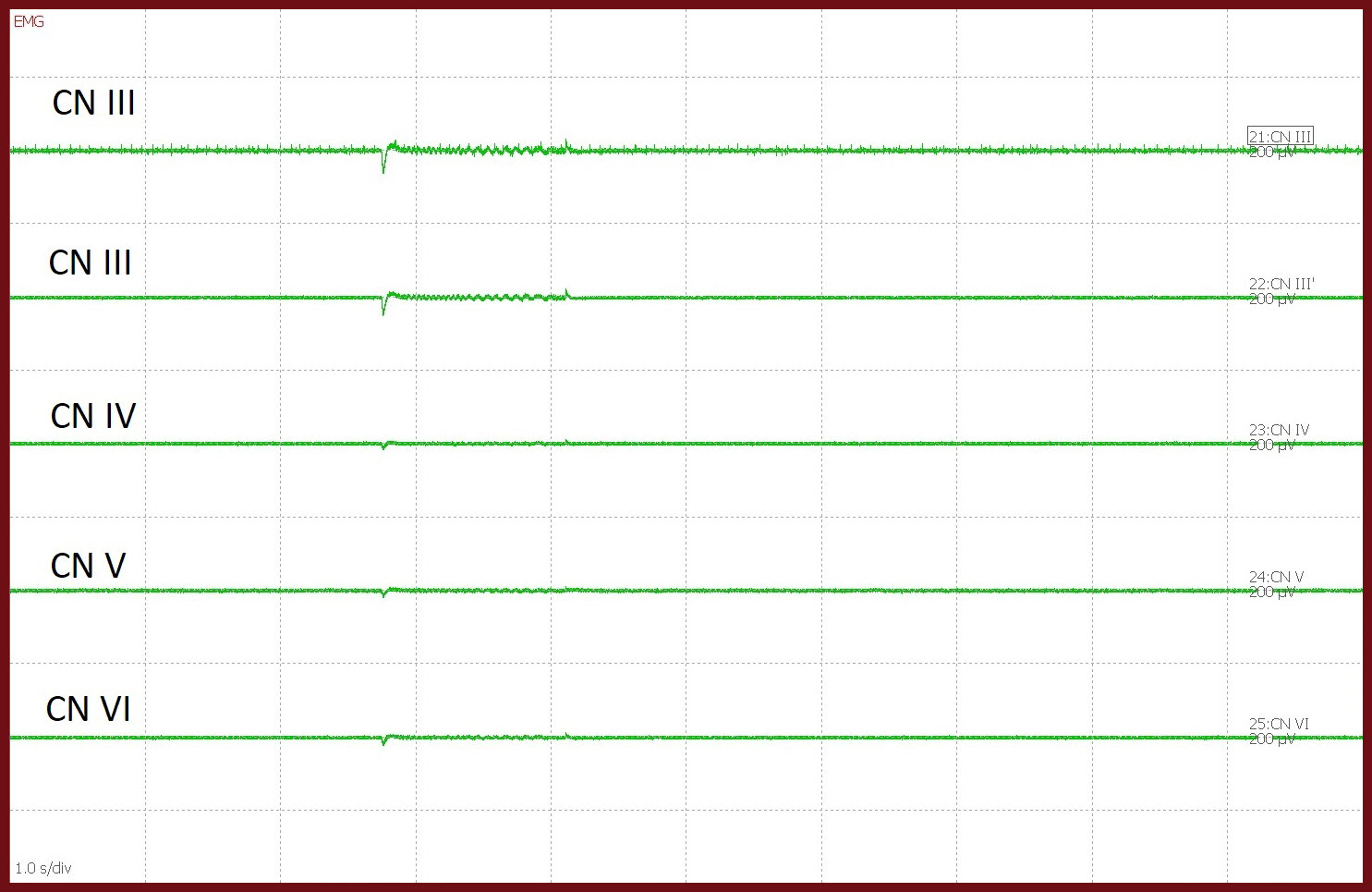
Fig 5. Left Infraorbital Trigeminal schwannoma resection. Upper cranial nerves spontaneous EMG (CN-sEMG) recorded from Medial Rectus (CN III), Inferior Rectus (CN III), Superior Oblique (CN IV), Masseter (CN V) and Lateral Rectus (CN VI) muscles.
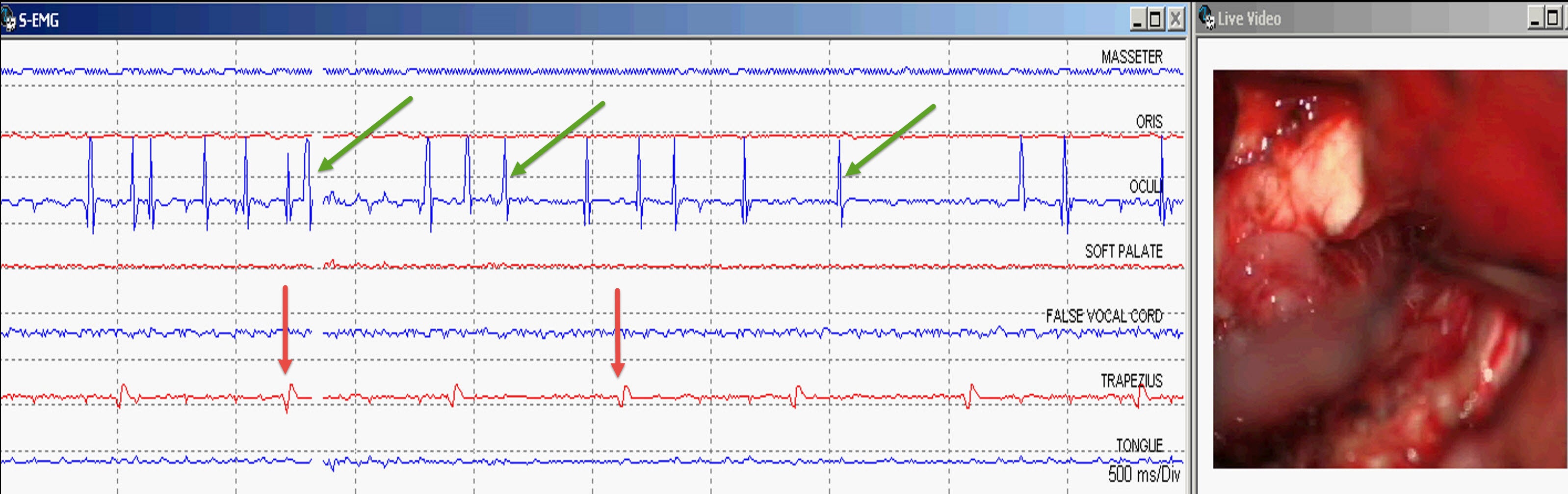
Fig 6: Right Cerebellopontine Angle (CPA) tumor resection. Left: Lower cranial nerves spontaneous EMG (CN-sEMG) recorded from Masseter (CN V), Orbicularis Oculi (CN VII), Orbicularis Oris (CN VII), Soft palate (CN IX), False Vocal Cords (CN X), Trapezius (CN XI) and Tongue (CN XII) muscles. Train EMG activity seen the Oculi muscle (green arrows) due to Facial nerve irritation. EKG artifact present in the left Trapezius muscle (red arrows). Right: Live video input from the microscope showing tumor resection.
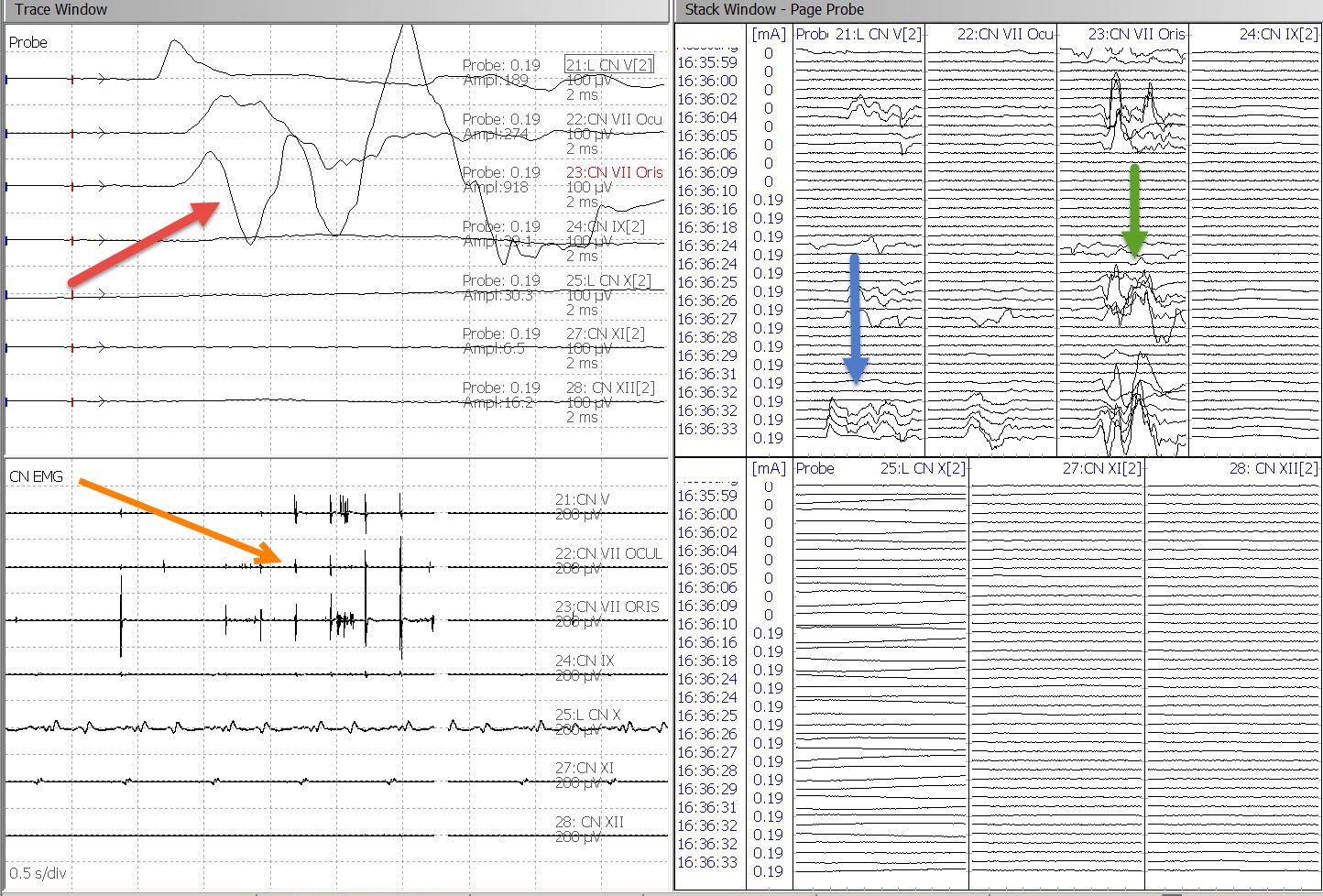
Figure 7. Left upper: Lower cranial nerves triggered EMG (CN-tEMG) responses recorded from Masseter (CN V), Orbicularis Oculi (CN VII), Orbicularis Oris (CN VII) (red arrow). Left Lower: Cranial nerves spontaneous EMG (CN-sEMG) showing response artifact (orange arrow). Right: Stack view of tEMG responses showing responses from CN V (blue arrow) and CN VII (green arrow)
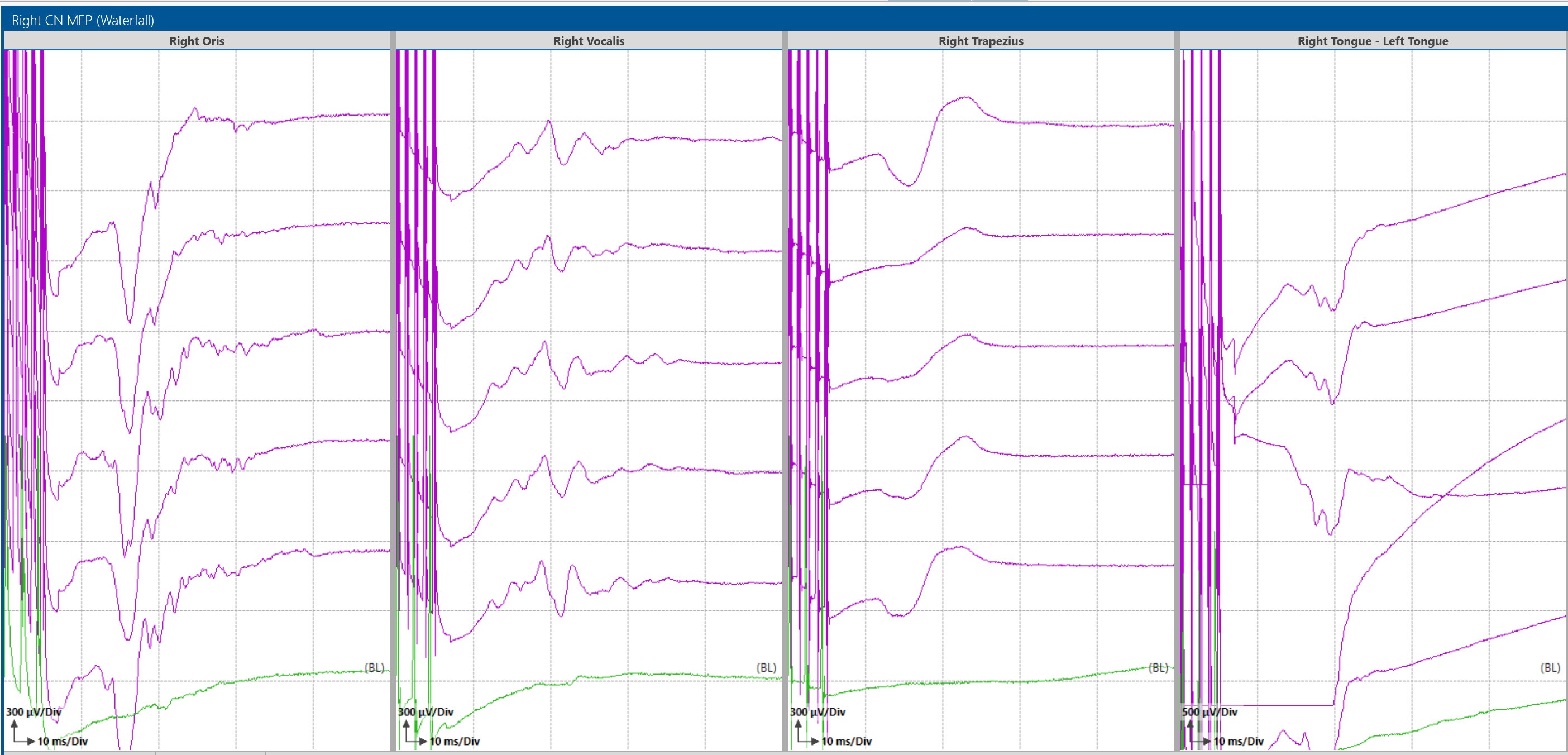
Figure 8: Corticobulbar Transcranial electrical motor Evoked Potentials (TCeMEP) recorded from Oris (CN VII), Vocal Cords (CN X), Trapezius (CN XI) and Tongue (CN XII) muscles during a fourth ventricle tumor resection.