

Recording Radial Nerve Somatosensory Evoked Potentials (Rn-SSEP) During Shoulder Surgeries
September 06, 2019
Faisal R. Jahangiri, M.D., CNIM, D.ABNM, FASNM, FASET1, Nida Qadir, MD2, James Blaylock, DC, CNIM1, Leah Cronce-Solano, CNIM1, Jason Ramsey, MD3
1Axis Neuromonitoring LLC, Richardson, TX, USA;
2APPNA, Association of Physicians of Pakistani Descent of North America, Westmont, IL;
3Dept. of Orthopedic Surgery, Grace Medical Center, Lubbock, TX.
A 76-year-old female patient presented with a left side periprosthetic humerus fracture, loosening of the implants and osteoporosis. Her past medical history included hypertension, borderline diabetes mellites, gout as well as multiple surgical procedures including hip replacement right knee replacement and left shoulder surgery. Her height was 144.78 cm,” and weight was 103.4 pounds.
Radiographic imaging showed no signs of healing of the humerus. Long-arm casting and non-operative measures did not show any signs of healing clinically. The surgeon decided to do an open reduction and internal fixation of the left shoulder joint. A multimodality Intraoperative Neurophysiological Monitoring (IONM) protocol was planned to include bilateral median nerve, radial nerve and posterior tibial nerve Somatosensory Evoked Potentials (SSEPs) (American Clinical Neurophysiological Society, 2009), bilateral upper and lower limb Transcranial electrical Motor Evoked Potentials (TCeMEPs), ipsilateral upper extremity electromyogram (EMG) and Train of Four (TOF). All the procedures were performed by a fellowship-trained orthopedic spine surgeon, with a CNIM (ABRET Neurodiagnostic Credentialing and Accreditation, 2019) certified technologist providing the neuromonitoring in the operating room,and a D.ABNM (ABNM: American Board of Neurophysiologic Monitoring, 2019) board-certified neurophysiologist available via remote-monitoring. A board-certified neurologist with a specialty in IONM was also present online during all surgical procedures.
We added radial nerve SSEP due to high risk of nerve damage (Sherfey & Edwards, 2009). There was a change in ipsilateral radial SSEP during the procedure with no changes in median nerve SSEP. The surgeon was immediately informed, and he released the retractors, and radial nerve SSEP came back to baselines within 20 min. Postoperatively, patient had no neurological deficits due to early identification of SSEP changes as well as quick intervention.
Radial nerve SSEP can be recorded along with median and ulnar nerves SSEP during these procedures with confidence.
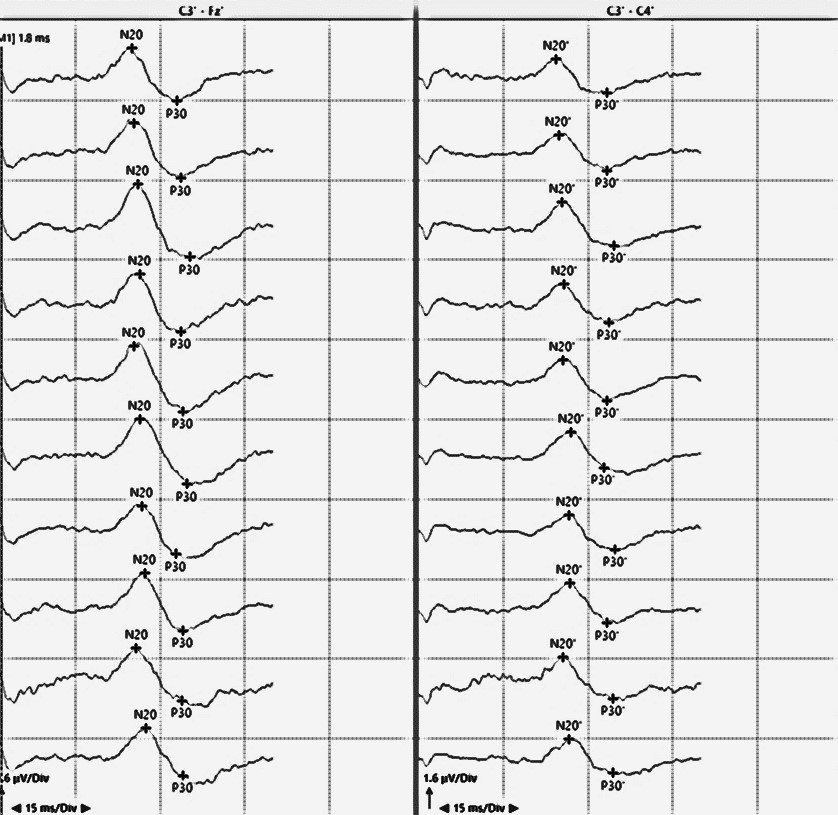
Figure: Reliable radial nerve somatosensory evoked potentials with cortical (CP3-FPz) and transcortical (CP3-CP4) responses recorded during a shoulder surgery.
References
ABNM: American Board of Neurophysiologic Monitoring. (2019, Sep 9). ABNM: American Board of Neurophysiologic Monitoring. Retrieved Sep 9, 2019, from ABNM: American Board of Neurophysiologic Monitoring: http://www.abnm.info/
ABRET Neurodiagnostic Credentialing and Accreditation. (2019, Sep 9). ABRET. Retrieved Sep 9, 2019, from ABRET: https://www.abret.org/candidates/credentials/cnim/
American Clinical Neurophysiological Society. (2009). https://www.acns.org/pdf/guidelines/Guideline-11B.pdf. Retrieved May 29, 2019, from ACNS. Guideline 11B: Recommended standards for intraoperative monitoring of somatosensory evoked potentials: https://www.acns.org/pdf/guidelines/Guideline-11B.pdf
Sherfey, M. C., & Edwards, T. B. (2009). Cement extrusion causing radial nerve palsy after shoulder arthroplasty: A case report. Journal of Shoulder and Elbow surgery, e21-e24.