

Train of Four (TOF) Monitoring: Are We Doing It The Right Way?
September 11, 2018
Faisal R. Jahangiri, MD, CNIM, D.ABNM, FASNM
Introduction:
In 1970, Ali et al. developed and published the technique of Train of Four (TOF) monitoring (Ali HH, 1970). TOF pattern was developed for assessing neuromuscular block in the anesthetized patient. TOF was developed as a stimulation pattern that did not require a comparison to a control response before administration of a neuromuscular blocking agent. It was done by stimulating the ulnar nerve with a TOF supra-maximal twitch stimuli:
· Frequency = 2 Hertz (Hz) for two seconds.
· Train frequency = 0.1 Hertz (every 10 seconds).
· Comparing T1 (1st twitch) to T0 (control)
· Comparing of T4 (4th twitch of the TOF) to T1 (known as the TOF ratio).
All patients who receive any neuromuscular blocking agents should be monitored for neuromuscular function during the surgeries. Face muscles are the first one to get paralyzed by muscle relaxants because they have better vascular supply followed by hand and feet. Face muscles are the first one to get four twitches back because of higher venous drainage as compared to hand and feet. Feet muscles are the last one to get paralyzed by muscle relaxants & the last one to get four twitches back (Gavrancic, Lolis, & Beric, 2014).
Physiology: Acetylcholine (Ach) is synthesized from Choline and Acetate and is stored in vesicles at motor endplates. Nerve impulse ends with Ach release into the cleft from these vesicles. Ach is then metabolized by Cholinesterase within milliseconds.
Muscle Relaxants: There are two types of muscle relaxants:
A. Depolarizers (DMR):
Succinylcholine is a depolarizing muscle relaxant ((DMR) with two Ach molecules acting like Ach at the post-synaptic receptor.
Characteristics:
· Phase I block: Decreases Single twitch, No fade (decrease but sustained response) to continuous stimulus, TOF ratio greater than 0.7, potentiation on anticholinesterase drugs, cause fasciculation.
· Phase II block: Resembles non-depolarizer blockade.
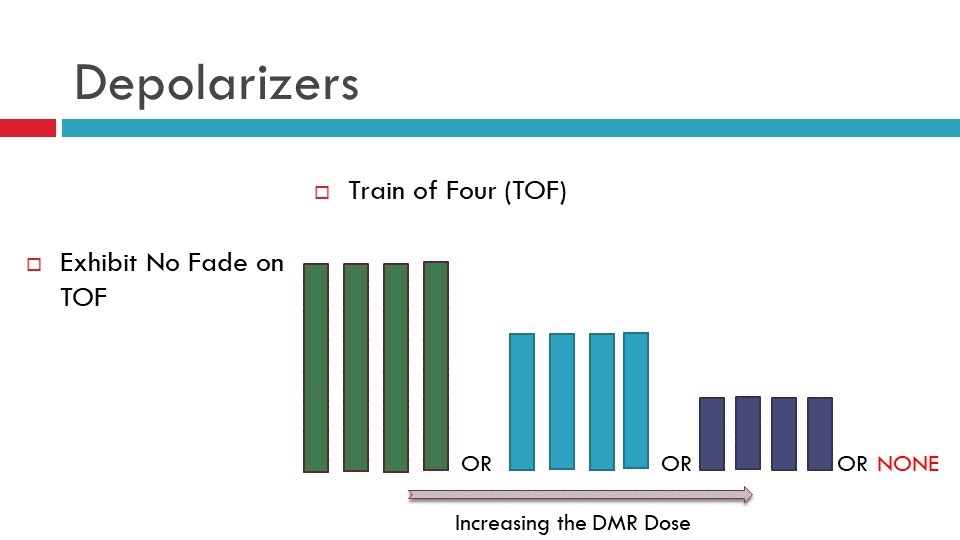
Figure 1. Depolarizing Muscle Relaxant (DMR) exhibit no fade on the Train of Four (TOF) test.
Non-Depolarizers (NDMR):
Curare, Pancuronium, Vecuronium, Rocuronium, Atracurium, Cis-Atracurium, Mivacurium, etc.
Characteristics:
An NDMR is a competitive antagonist that blocks conduction by acting on alpha subunit. decrease twitch response to a single stimulus. NDMR produces fade (unstained response) to continuous stimulus. For NDMR the TOF ratio is less than 0.7 (T4 is less than 70% amplitude of T1). It causes post-tetanic facilitation, potentiation by other non-depolarizers, antagonism by anticholinesterase drugs.
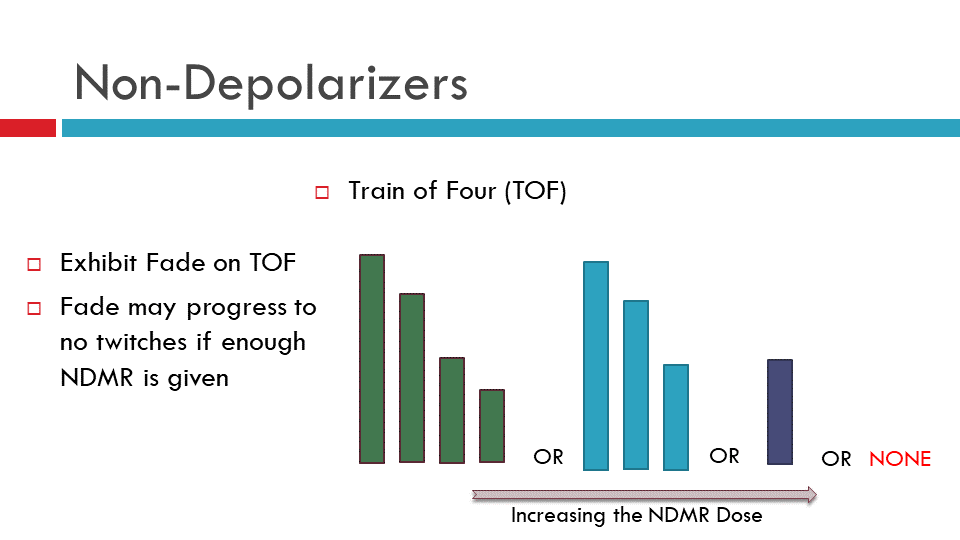
Figure 2. Non-Depolarizing Muscle Relaxant (NDMR) exhibit fade on the Train of Four (TOF) test. This image presents fade in TOF responses.
Why give muscle relaxation?
1) For adequate intubation
2) For adequate surgical exposure
3) To improve mechanical ventilation
Why monitor Neuromuscular Junction (NMJ)?
· Due to variable individual response to muscle relaxants.
· Because of the narrow therapeutic window.
· There is no detectable block until 65 to 75% of receptors are occupied.
· Paralysis is complete at 90 to 95% receptor occupancy.
· Therefore, adequate muscle relaxation corresponds to a narrow range of 85 to 90% receptor occupancy.
Clinical application (level of muscle relaxation):
· Surgical Relaxation at >90%
· Intubation facilitated at 95%
· Total Flaccidity at 99%
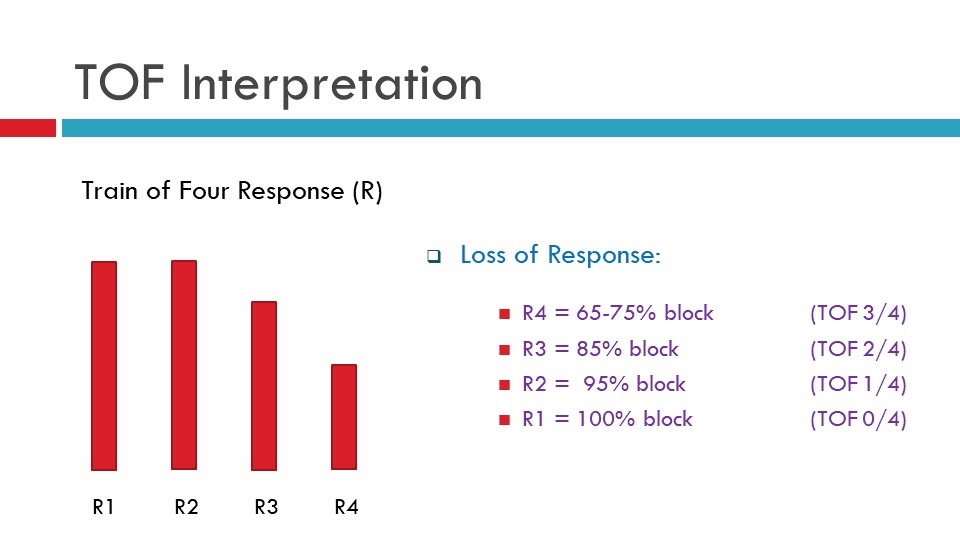
Figure 3. Train of Four (TOF) Interpretation: A presence of 4th twitch = 0-5% paralysis, 3rd twitch = 65-75% paralysis, 2nd twitch = 85% paralysis, 1st twitch = 95% paralysis, 0 twitch = 100% paralysis.
Objective:
· Post-operative muscle relaxant occurs even with intermediate-acting NDMR agents.
· Satisfactory recovery has not occurred from NMB until the TOF ratio is >0.9.
· Onset and recovery from NMB occur at different rates in different muscles.
· Intraoperative TOF monitoring is needed from appropriate muscles to make sure the EMG monitoring is reliable.
Patient Setup for TOF:
Types of NM stimulators:
1) Single Twitch
2) Tetanic Stimulation
3) Train of Four Stimulation
· Always setup the most distal muscle,
· Make sure your stimulation and recording setup is correct.
· If you are not getting TOF from one side, try the contralateral side.
· TOF should be done throughout the surgical procedure.
· Keep the intensity to a minimum.
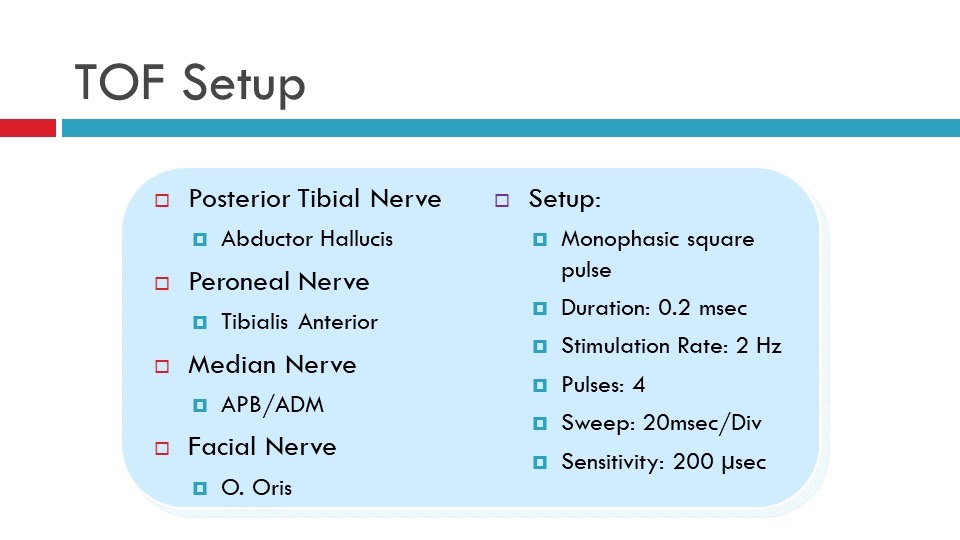
Figure 4. Train of Four (TOF) setup: Stimulation and recording sites with stimulation and recording parameters (Jahangiri, Faisal R, 2012, Surgical Neurophysiology,2nd Edition).
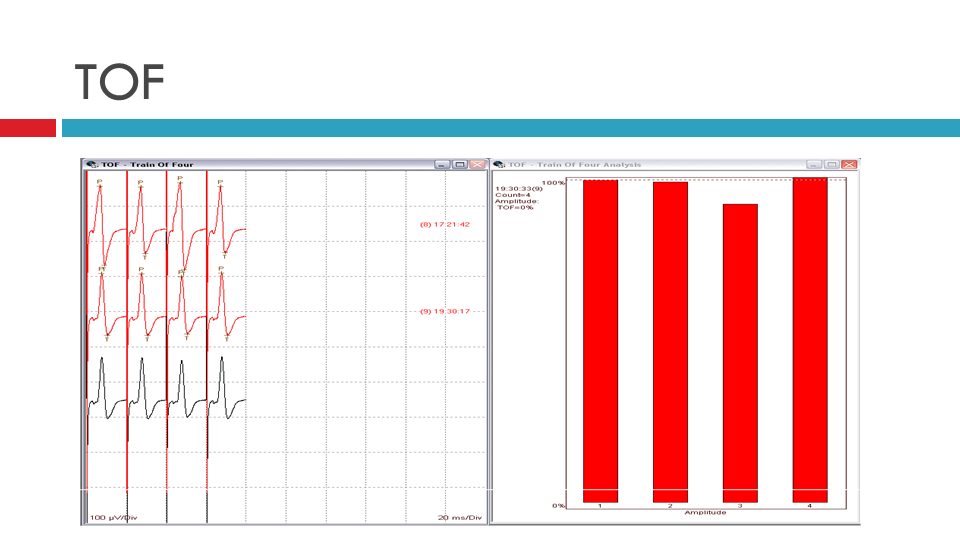
Figure 5. Train of Four (TOF): Left: data showing all four twitches present. Right: TOF representation in the histogram view.
Factors affecting TOF:
· Calcium Channel Blockers
· Corticosteroids
· Diuretics (furosemide and thiazides)
· Carbamazepine
· Enflurane and Isoflurane (inhalants)
· Antibiotics (Amikacin, Clindamycin, Gentamycin, Kanamycin, Neomycin, Piperacillin, A, B and E, Streptomycin, Tetracycline and Tobramycin)
· Anti-arrhythmic medications (Bretyllium, Lidocaine, Propranolol, Quinidine)
· Electrolyte and thermal disorders (Hypokalemia, Hypocalcemia, Hypomagnesaemia, Hyponatremia, Hypothermia, Acidosis)
· Organ Failure (renal and hepatic)
· Neuromuscular diseases (Myasthenia Gravis, Bell’s Palsy)
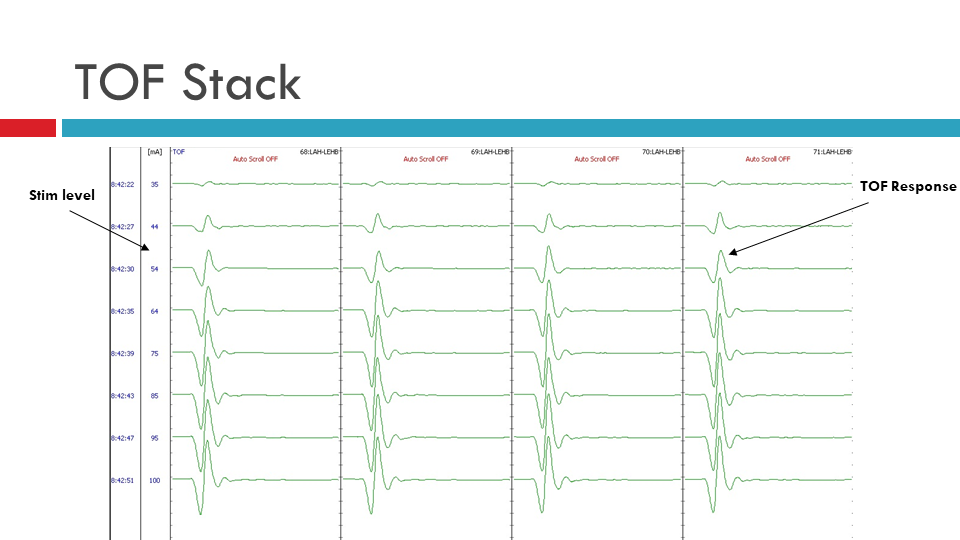
Figure 6. Train of Four (TOF) Stack: Data showing all four twitches present in stack format ranging from 35 mA (top) to 100 mA (bottom).
Why do we need to do TOF correct way?
· Interpreting the responses correctly to avoid false negative:
o Pedicle screw stimulation threshold
o Peripheral nerve stimulation threshold
o Cranial nerve stimulation threshold
o MEP stimulation threshold & interpretation
o Cortical Mapping stimulation threshold
o Dorsal Root Rhizotomy (SDR) stimulation threshold
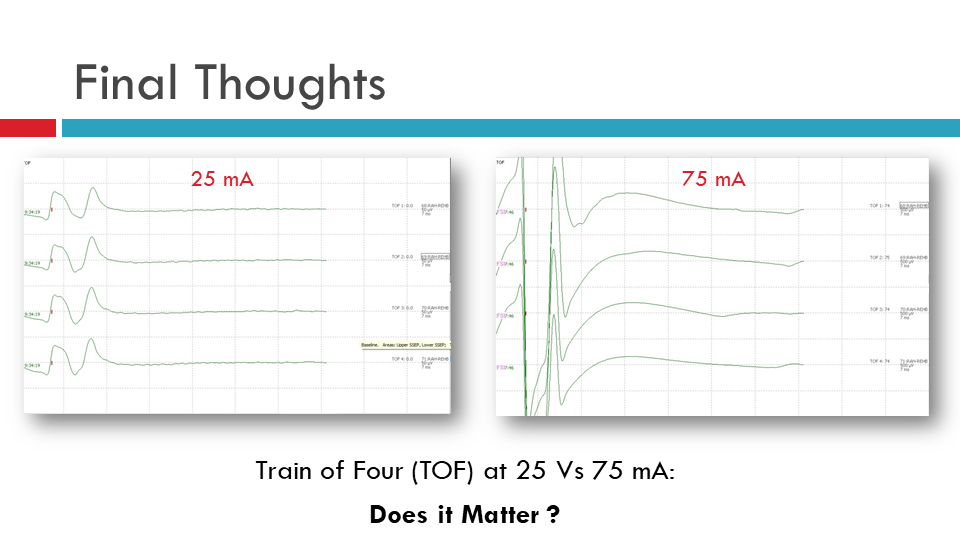
Figure 7. Train of Four (TOF) data comparison for TOF at 25 mA versus TOF at 75 mA.
References
Ali HH, U. J. (1970, Nov). Stimulus frequency in the detection of neuromuscular block in humans. Br J Anaesth, 42(11), 967-78. Retrieved Sep 07, 2018, from https://bjanaesthesia.org/article/S0007-0912(17)50404-3/pdf
Gavrancic, B., Lolis, A., & Beric, A. (2014, Dec). Train-of-four test in intraoperative neurophysiologic monitoring: differences between hand and foot train-of-four. Clin Neurophysiol, 31(6), 575-9. doi:10.1097/WNP.0000000000000111
Jahangiri, F. R. (2012, Apr)). Surgical Neurophysiology 2nd Edition: A Reference Guide to Intraoperative Neurophysiological Monitoring (2nd ed.). Charleston, SC: CreateSpace Independent Publishing.