Utilizing longer intramuscular needle pair electrodes:
April 16, 2018
What are we really missing in our Intraoperative Muscle Recordings?
(Paper was presented by Dr. Faisal Jahangiri at the 2015 annual meeting of American Society of Neurophysiological Monitoring (ASNM) in Chicago, Illinois. It received a Lead Author-Scientific Achievement Award from the ASNM research committee). Dr. Jahangiri also presented this paper at the 2015 annual meeting of American Neurodiagnostic Society (ASET) in Weston, Florida.
Objective:
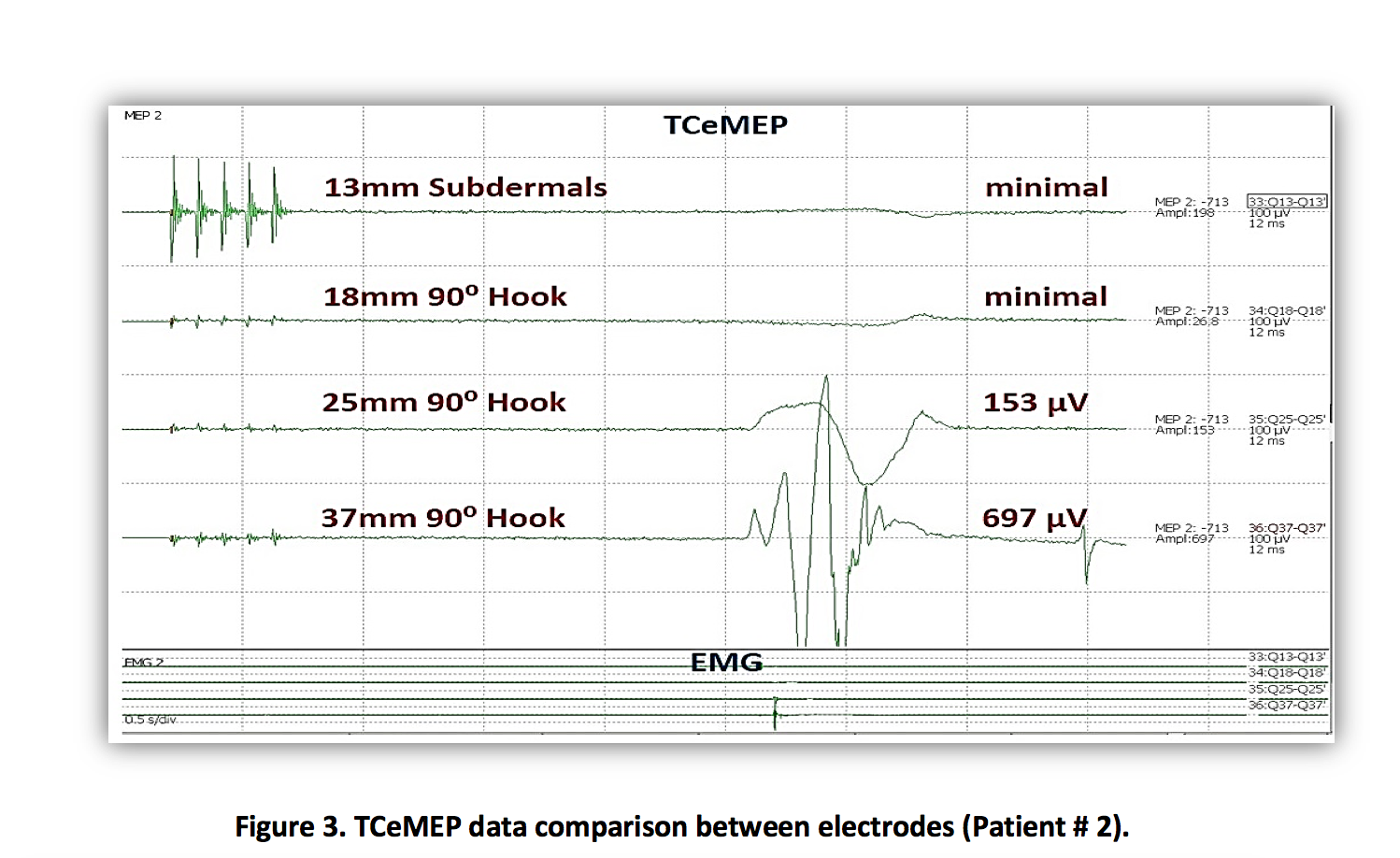
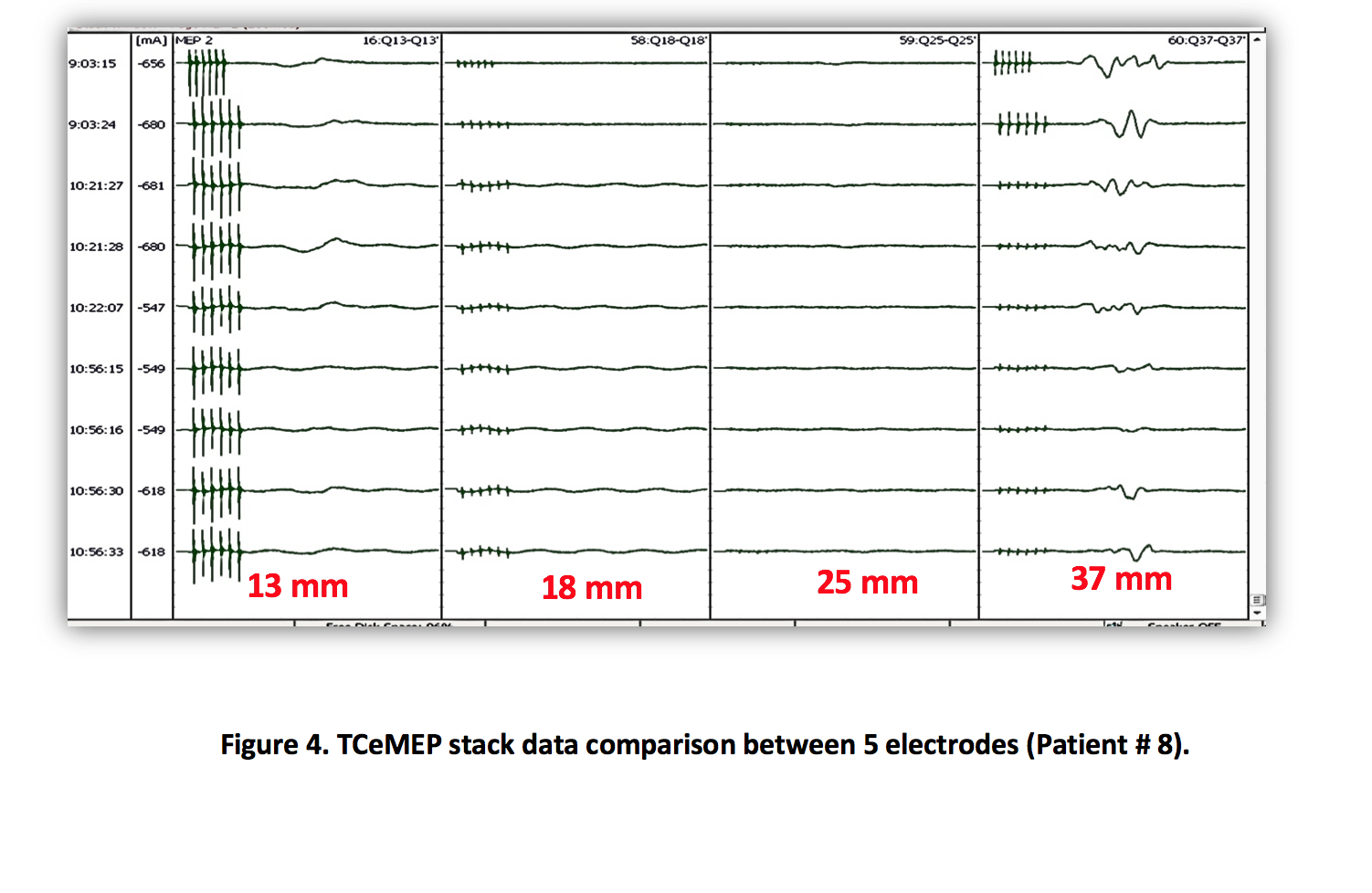
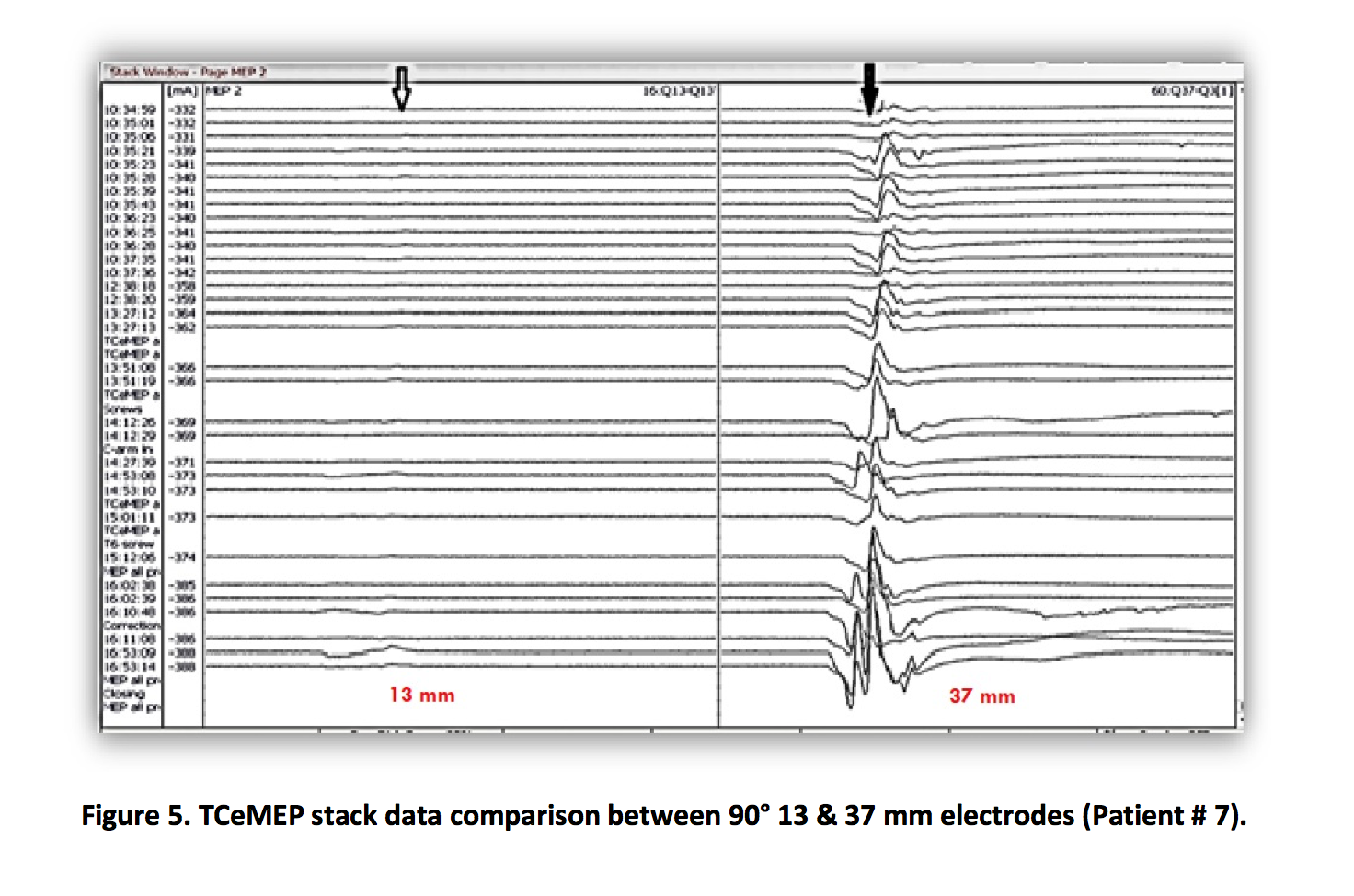
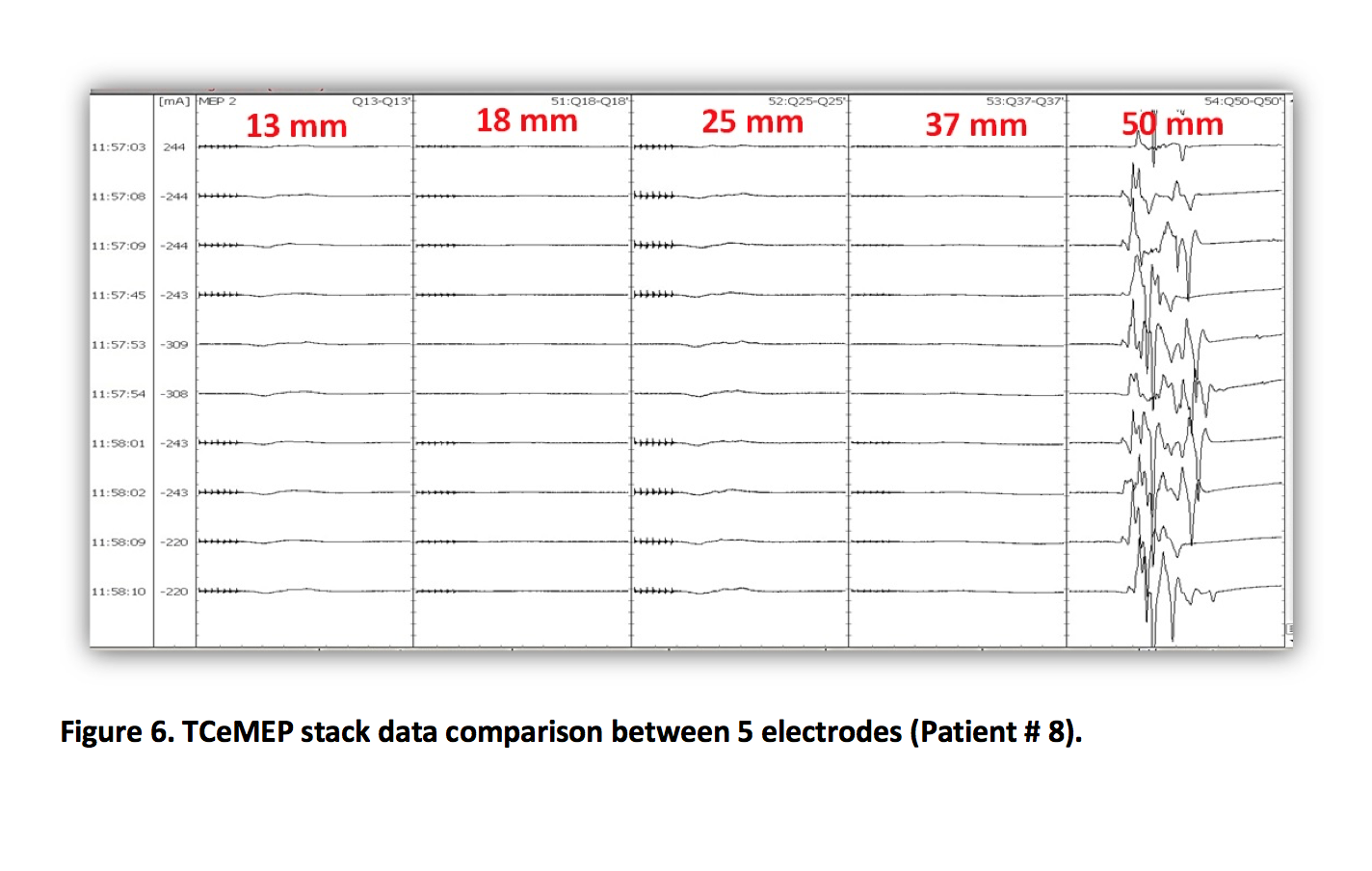
This study illustrates the benefit of utilizing longer 37mm and 50mm intramuscular needle pair electrodes for recording Transcranial electrical Motor Evoked Potentials (TCeMEP) in Rectus Femoris (RF) muscle during various surgeries in obese patients, as opposed to the regularly used sub-dermal 13 mm needle electrodes, which can miss muscle activity (EMG) due to presence of adipose tissue. The 37 mm and 50mm intramuscular needle pair electrodes increased accuracy and reliability of TCeMEP recording at lower stimulation thresholds.
Methods:
We performed a retrospective review of spinal neurophysiological monitoring cases at the King Abdulaziz Medical City, Riyadh, Saudi Arabia. Our recording setup included 13, 18, 25, 37 and 50 mm long 90 degree intramuscular needle pair electrodes placed in right Rectus Femoris muscle. This setup was in addition to somatosensory evoked potentials (SSEP), TCeMEP and EMG from all four extremities muscles. Train of four (TOF) was used as well for monitoring the level of muscle relaxant.
Results:
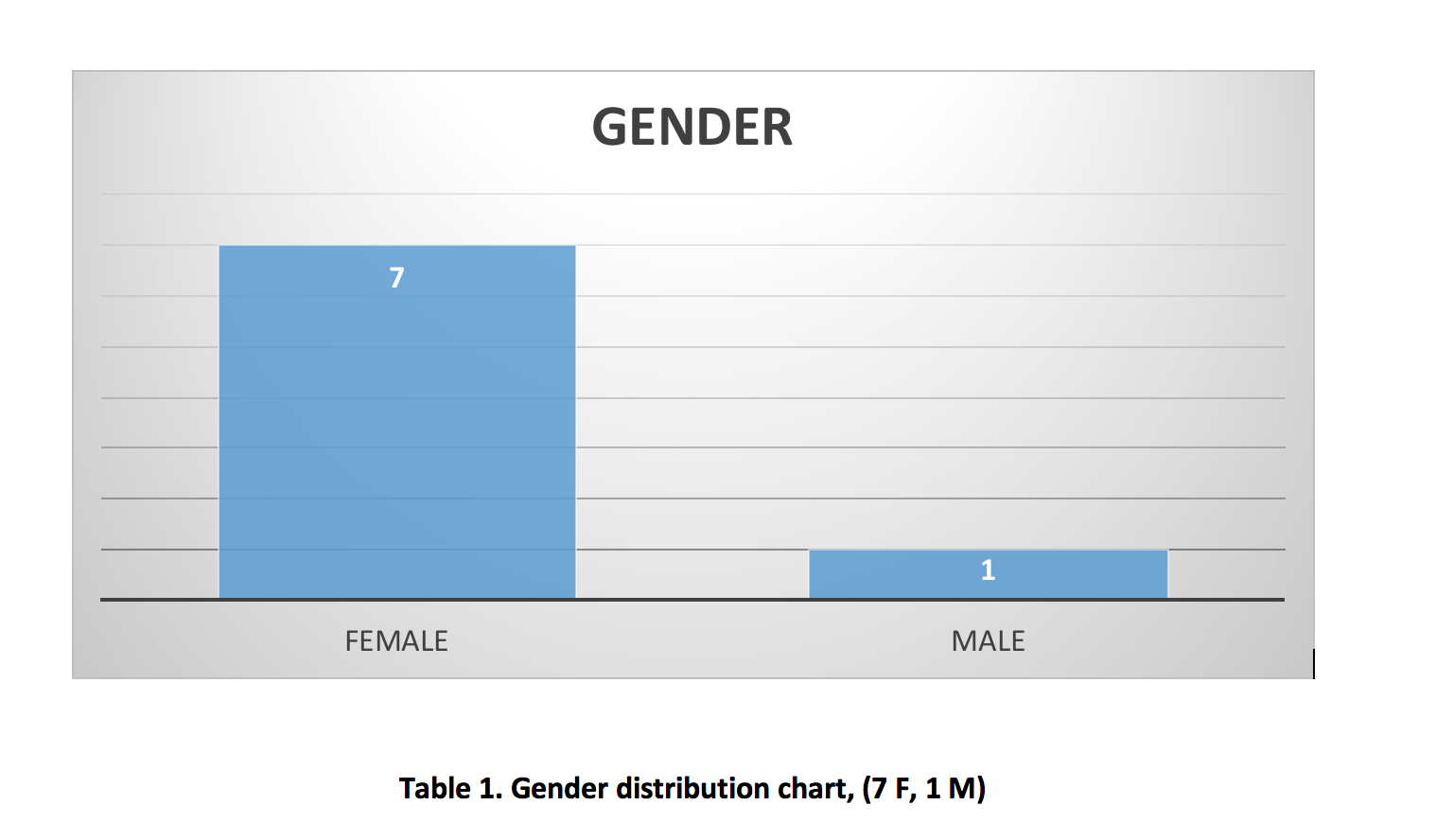
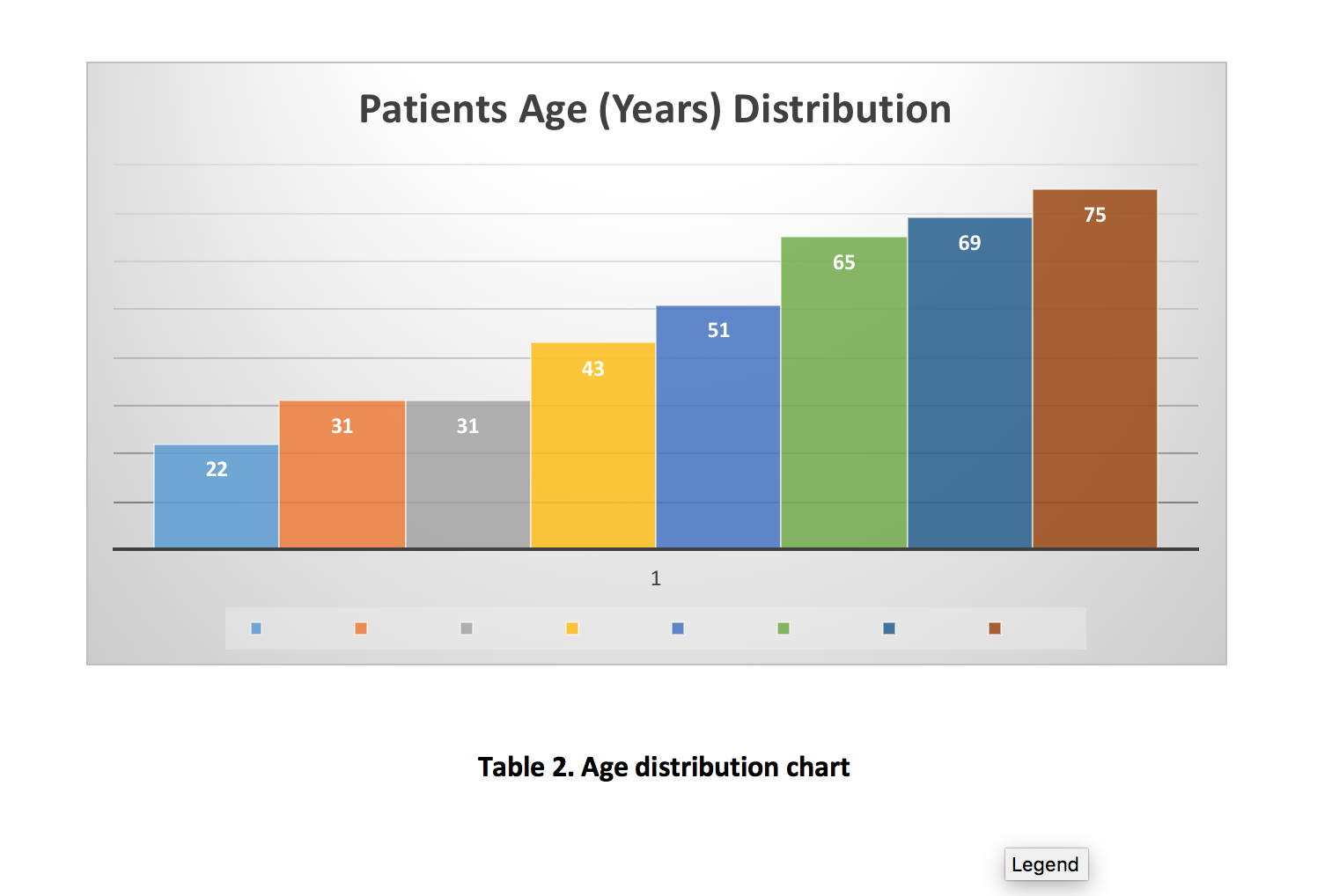
Eight consecutive cases were identified. The patients consisted of seven females and one male with age ranging from 22 to 75 years (median: 48 years). Two patients had a spinal tumor, one of each patient had scoliosis, spinal fracture, cranio-cervical compression, hyper-kyphosis, cervical spine stenosis, and one spondylolisthesis. The TCeMEP thresholds ranged from 120–280 Volts (median: 160 V). TCeMEP recordings were recorded in all seven patients with 37 mm hook recordings and one patient with 50 mm hook electrode recording (100%). On the other hand, TCeMEP were recordable only in one patient with 13 mm sub-dermal needle recordings (12.5%).
Conclusions:
Our muscle recordings with 37 mm and 50 mm length intramuscular needle pairs were much more reliable than 13 mm sub-dermals in obese patients. These long intramuscular needle pair electrodes are more secure and allow for lower stimulation intensities reducing the risks of excessive TCeMEP stimulation.
Acknowledgements:
Special thanks to Brett Netherton, MS, CNIM, FASNM; Patty Warf, MS, RN, CNIM of Signal Gear, LLC, USA and Abdullah AlBishi, R.EEGT and Ahmed Alanizi, Neurophysiology Lab, Division of Neurology, King Albdulaziz Medical City, Riyadh, Saudi Arabia for providing their valuable support for this study.

Figure 1. 13, 18, 25, 37 and 50 mm long 90 degree intramuscular needle pair electrodes (Courtesy: Signal Gear LLC, USA)
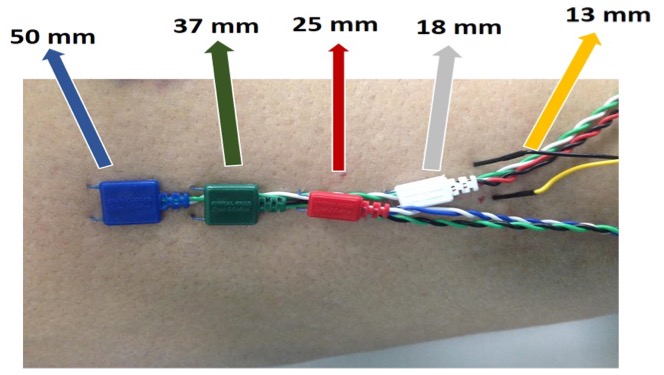
Figure 2: All Electrodes placed on right Rectus Femoris muscle. Left: Head; Right: Foot (Patient # 3).